Article Text

Abstract
Objective To estimate associations between trivalent influenza vaccination and COVID-19 mortality as well as severe clinical outcomes among hospitalised patients.
Design Retrospective observational study.
Setting This study was conducted among hospitalised patients with COVID-19 in Brazil.
Participants We analysed all hospitalised patients with COVID-19 with available vaccination information captured in Brazil’s national electronic respiratory infection data system between 1 January 2020 and 23 June 2020.
Main outcome measures The primary outcomes were age-specific mortality rates of hospitalised patients with COVID-19 with and without recent inactivated trivalent influenza vaccination.
Results A total of 53 752 clinically confirmed COVID-19 cases were analysed. Controlling for health facility of treatment, comorbidities as well as an extensive range of sociodemographic factors, patients who received a recent influenza vaccine experienced on average 7% lower odds of needing intensive care treatment (95% CI 0.87 to 0.98), 17% lower odds of requiring invasive respiratory support (95% CI 0.77 to 0.88) and 16% lower odds of death (95% CI 0.78 to 0.90). Protective effects were larger when the vaccine was administered after onset of symptoms as well as among younger patients.
Conclusion Patients with COVID-19 with recent inactivated influenza vaccination experience significantly better health outcomes than non-vaccinated patients in Brazil. Beneficial off-target effects of influenza vaccination through trained innate immune responses seem plausible and need to be further explored. Large-scale promotion of influenza vaccines seems advisable, especially in populations at high risk for severe COVID-19 disease progression.
- immunisation
- infectious disease medicine
Data availability statement
Data are publicly available at the Brazilian Ministry of Health website.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Summary box
What is already known about this subject?
We searched PubMed, BioRxiv and MedRxiv for articles published in English from inception to 30 June 2020, with the following terms: “Covid-19”, “SARS-CoV-2” AND “influenza”, “flu” AND “vaccine”, “vaccination”.
While the potential benefits of influenza vaccines have been highlighted in several theoretical commentaries, modelling studies, notes and letters, only two small empirical studies were found.
The first study shows that on average countries with higher influenza vaccination coverage have lower COVID-19 incidence and mortality.
A second study found a similar relationship when looking at county-level outcomes in the USA.
No study was found analysing patient-level data.
Summary box
What are the new findings?
This is the first study assessing the associations between influenza vaccination and COVID-19 severity as well as COVID-19 mortality using clinical patient records.
The data set used allows us to control for a large number of potentially confounding factors including age, race, gender, pre-existing health conditions, quality of healthcare and socioeconomic status.
We show that conditional on all of these factors, patients with a recent influenza vaccination are more likely to survive COVID-19 and less likely to need intensive care or respiratory support.
How might it impact clinical practice in the foreseeable future?
Concerns regarding potential negative side effects of influenza vaccination in the context of SARS-CoV-2 infections seem unwarranted.
Large-scale promotion for increased uptake of influenza vaccines seems advisable, especially in high-risk groups for severe SARS-CoV-2 infections.
Lowering the overall burden of respiratory viral infections during the influenza season will preserve test and care capacity for patients in greatest need, and, importantly, will also reduce the risk for nosocomial SARS-CoV-2 transmission.
Introduction
As of 1 July 2020, COVID-19 had affected over 10 million individuals globally and caused an estimated 506 064 deaths.1 Many countries south of the equator are now entering the cold season of the year, which will likely result in a substantial increase in patient volume due to influenza. Seasonal influenza outbreaks occur in regular intervals in most non-tropical countries, and cause an estimated 650 000 deaths each year.2 Despite major public health efforts, influenza vaccines remain underused in most countries due to scepticism regarding their efficacy and concerns surrounding their safety.3 4 Several social media rumours linking influenza vaccine to adverse COVID-19 outcomes in recent weeks5 have further undermined the willingness of the general population to undergo influenza vaccination.
SARS-CoV-2 and influenza viruses are both enveloped RNA viruses that share common transmission and routes of entry and demonstrate largely overlapping clinical features. Three recent studies have documented a negative correlation between influenza vaccination coverage and COVID-19 mortality at the country level,6 across Italian regions7 as well as across counties in the USA.8 In this paper, we use detailed medical records from over 50 000 hospitalised patients with COVID-19 in Brazil to assess whether such protective associations can be identified at the patient level.
Methods
Study design
The study was designed as a clinical cohort study following all hospitalised patients with confirmed COVID-19 diagnosis registered in Brazil between 1 January 2020 and 23 June 2020.
Setting
The study was conducted in Brazil, the sixth most populous country in the world, with an estimated population of 212 million in 2019. As of 1 July, Brazil is the country with the second highest number of COVID-19 cases, as well as the country with the largest number of new deaths documented each day (https://coronavirus.jhu.edu/map.html).
Influenza vaccine campaign
The Brazilian Ministry of Health (MoH) has been conducting annual vaccination campaigns achieving relatively high population coverage since 1999.9 10 Seasonal influenza in Brazil usually peaks in April and May in northern, and in June and July in southern states.11 The 2020 annual influenza vaccination campaign was launched on 23 March, 1 month earlier than originally planned to ensure vaccine delivery to the public prior to the incoming wave of SARS-CoV-2 infections, with the ambition to reach a total of 67.6 million people nationwide.12 The national campaign targets senior citizens (aged 60 and older) and health workers in phase I; patients with chronic or other clinical conditions, teachers and security forces in phase II and children and other high-risk populations in phase III.12 Based on the recommendation from WHO, a trivalent (type A/Brisbane/02/2018—IVR-190 (H1N1), type A/South Australia/34/2019—IVR-197 (H3N2) and type B/Washington/02/2019), non-adjuvant influenza vaccine produced in Brazil by the Instituto Butantan is currently used.13
Data sources
All data used were collected within the Brazilian Surveillance System for Severe Acute Respiratory Infections (‘Vigilância de Síndrome Respiratória Aguda Grave’ (SRAG)). Since 2009, Brazil operates a national disease surveillance network, which requires all health facilities and providers to report all severe respiratory infections treated at health facilities into a central system using a standardised reporting protocol. The COVID-19 pandemic is considered a national public health emergency, which requires that all cases must be reported within 24 hours to the MoH. In compliance with Brazilian public law (Lei 12.527/2011, art. 7, § 3°), the MoH makes these surveillance data publicly available, after removing all identifiable information.
Participants
All hospitalised individuals with a clinical COVID-19 diagnosis registered in the SRAG system between 1 January 2020 and 23 June 2020 were analysed. According to Brazilian law, all hospitals need to complete a case report form for individuals with severe respiratory infection. Patients are classified as having a respiratory infection if they have at least two out of the following symptoms: fever, chills, sore throat, headache, cough or loss of smell or taste. The respiratory infection is classified as severe if the patients additionally presents respiratory difficulty OR persistent chest pressure OR oxygen saturation <95% OR bluish colour of the lips or face.
Variables
All data used are collected through a standard case report form developed by the Brazilian Ministry of Health. This form is available at: https://opendatasus.saude.gov.br/dataset/ae90fa8f-3e94-467e-a33f-94adbb66edf8/resource/54a46c6d-e0b5-40b7-8b74-85450d22ace3/download/ficha-srag-final-27.07.2020_final.pdf. The form contains 80 fields, and covers a range of patient characteristics as well as clinical variables. Our primary outcome variable was patient survival; we also analysed intensive care treatment as well as invasive respiratory support as (intermediate) secondary outcomes. Our primary exposure of interest was vaccination status. As part of the standard patient questionnaire, patients are asked if they got vaccinated in the most recent influenza vaccination campaign (‘Recebeu vacina contra Gripe na última campanha?’). If the patient did, the vaccination date is also entered in the system. In addition to the vaccination information and the clinical outcomes, we extracted the following covariates from the system: age, sex, race, educational attainment, treatment facility and prior diagnosis with cardiovascular conditions, haematological conditions, liver problems, asthma, diabetes, neurological disorders, respiratory conditions, renal conditions, immune-suppression and obesity. The complete codebook underlying the data set used is available in the online supplemental materials and can also be directly accessed at the Ministry’s webpage at https://opendatasus.saude.gov.br/dataset/ae90fa8f-3e94-467e-a33f-94adbb66edf8/resource/8f571374-c555-4ec0-8e44-00b1e8b11c25/download/dicionario-de-dados-srag-hospitalizado-27.07.2020-final.pdf.
Supplemental material
Bias
The primary bias concern for our analysis is confounding; we addressed this concern by controlling for a large number of covariates as outlined in the ‘Statistical methods’ section. There is also a potential bias in the study because patients whose vaccination status was not documented in the medical record were excluded from the analysis. While there are currently no studies assessing the reasons for incomplete reporting in the SRAG system, it seems likely that complete reporting is more common at better endowed or more motivated facilities. This should not undermine the internal validity of the study, but means that the estimates presented are not necessarily representative of all Brazilian patients. There is also potential misclassification bias if the diagnosis is not based on a laboratory testing—we addressed this in our analysis by restricting the sample to patients where laboratory tests were available.
Statistical methods
We start by presenting sociodemographic characteristics of patients, as well as the proportion of patients requiring intensive care and respiratory care by gender, age, education and race. In a second step, we plot average survival probabilities for vaccinated and non-vaccinated individuals by 10-year age group.
In a third step, we use multivariable regression models to estimate the associations between vaccination status and health outcomes. Our primary analysis focuses on the full sample of patients where both vaccination and survival data were available. We first present empirical models that control for age and use within-facility variation only (logistic regressions conditioned on treatment facility). To further control for potential differences in disease severity, we show models that control for an extensive list of comorbidities documented in the clinical records. We also show models that control for educational attainment and race to address concerns regarding selective vaccination uptake within facilities. Last, we restrict our sample to individuals with a confirmed positive SARS-CoV-2 PCR test (subsample analysis). For our secondary outcomes (intensive care treatment and respiratory support), we once again restrict the sample to those patients where both vaccination status and these outcomes are available.
Last, in order to investigate the role of timing of vaccine administration, we divided patients with recent influenza vaccination into three groups: patients receiving the vaccine after onset of symptoms; patients receiving the vaccine as part of the 2020 campaign (in March 2020 or later), but prior to the onset of symptoms and patients receiving the vaccine as part of earlier campaigns. We used models with a complete set of controls to assess the associations of these different subgroups with mortality outcomes first in the full sample, and then separately estimated models among individuals under age 60, and individuals age 60 years and older.
To allow for clustering of residuals at the facility level, the Huber-White cluster-robust variance estimator was used in all empirical models. All analyses were conducted using the Stata SE V.16 statistical software package.
Missing data
To address missingness in the covariates included in the analysis multiple imputation using chained equations was applied. We used Stata’s MI package to generate 100 randomly imputed datasets for our analysis. With the regress option used, the package fills in missing values of a continuous variable using the Gaussian normal regression imputation method. Observations with missing outcome data (patients still in treatment: n=25 235) or missing data on vaccination status (n=56 014) were excluded from the analysis. Missing data on all other covariates were imputed using multiple imputations with chained equations.
Results
A total of 53 752 hospitalised COVID-19 cases were analysed. Fifty-seven percent of patients were male, and the median age of patients was 56 years (table 1); 79.8% of these patients had a documented positive SARS-CoV-2 PCR test. The most represented age groups among patients with COVID-19 were individuals between 50 and 59 years of age. Twenty-nine percent of patients received intensive care, 16% were given invasive respiratory support and 46.5% of patients died. COVID-19 fatality rates increased from 12.7% among children under the age of 10 years to 79% among individuals above 90 years (table 1); 59.4% of patients with COVID-19 had a pre-existing cardiovascular condition and 49.3% had previously been diagnosed with diabetes mellitus. The prevalence of obesity, renal disease and respiratory conditions were 9.2%, 8.6% and 7.6%, respectively (online supplemental material figure S1).
Severity and mortality outcomes of patients with COVID-19 by gender, age, race and educational attainment
Online supplemental materials figure S2 illustrates vaccination coverage by age; 31.2% of patients received an influenza vaccine overall. Rates were substantially higher among children under age 6 years as well as adults aged 60 years and above, but were below 50% in all age groups in our population analysed here.
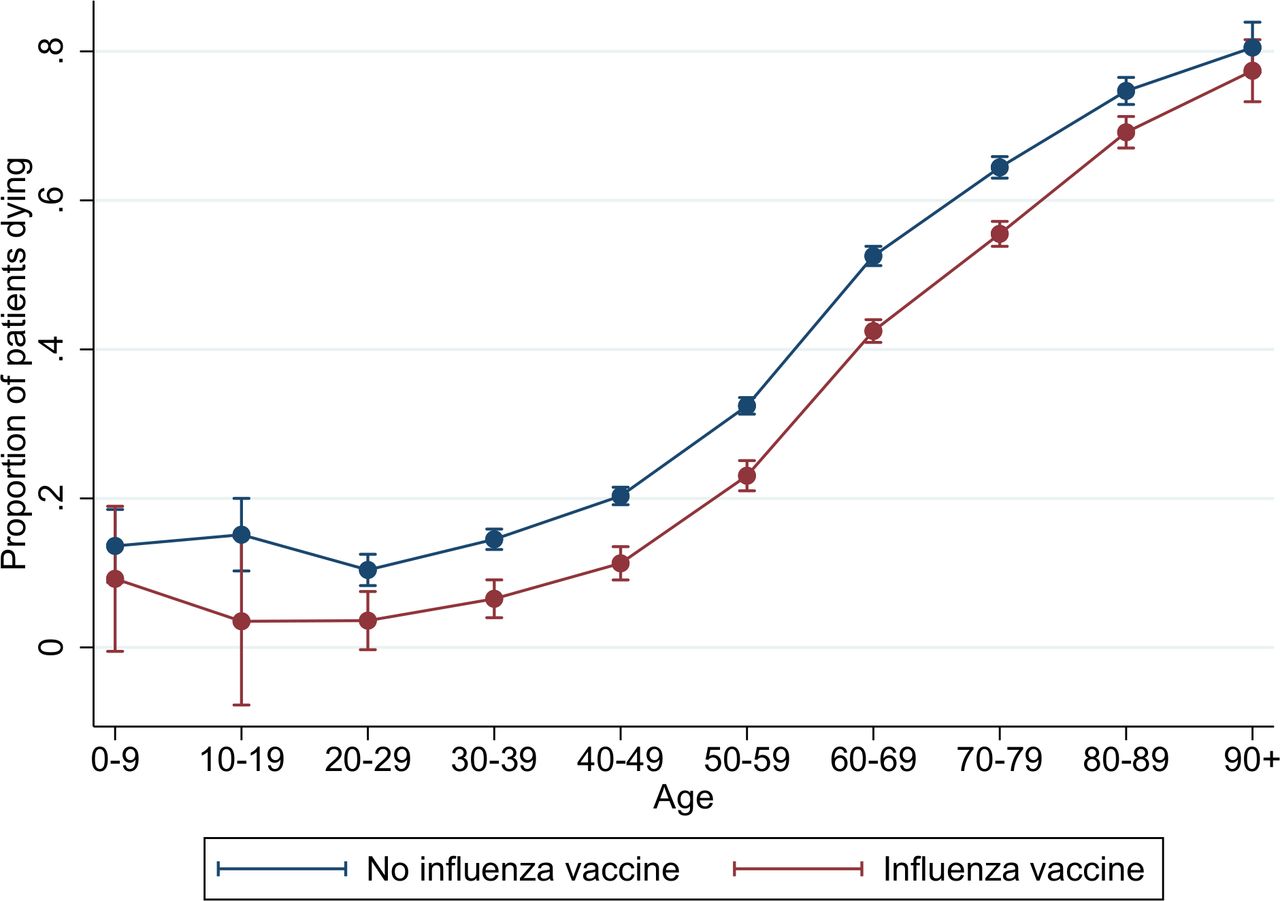
Figure 1 shows mortality patterns by age and vaccination status. COVID-19-related mortality ranged from 14% among children under the age of 10 years to 81% among individuals aged 90 years or older in the non-vaccinated group. Mortality was consistently lower among influenza vaccinated patients across all age groups, with absolute mortality differences ranging from a risk difference of 12% patients in the 10–19 age group to a risk difference of 3% patients in the 90+ age group. This difference was statistically significant (p<0.05) for all age groups between 30 and 90 years.
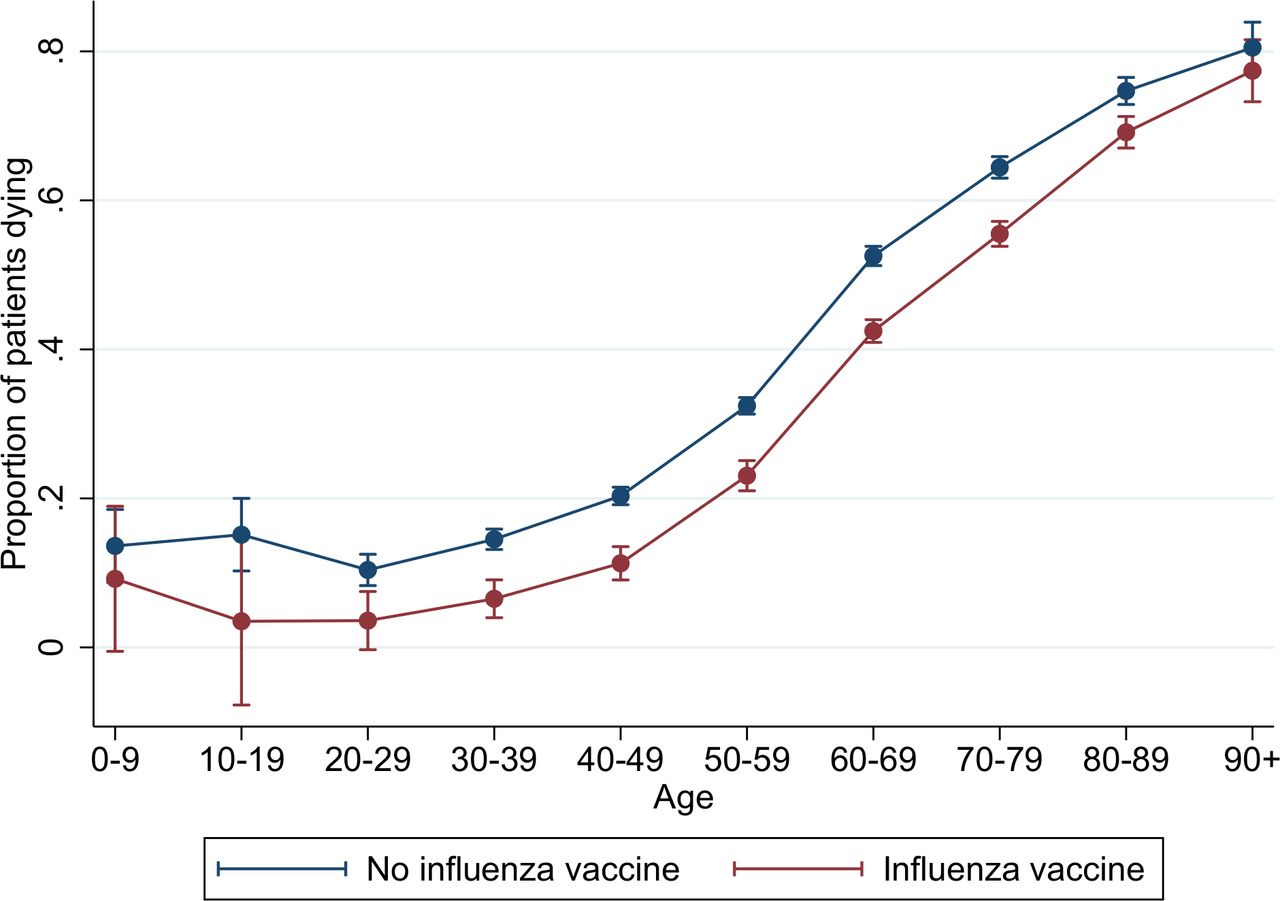
COVID-19 mortality by age and vaccination status. The proportion of patients with COVID-19 dying by age group and influenza vaccination status. Based on a sample of 40 394 cases with observed mortality outcomes. Estimates represent unadjusted linear differences in age group-specific mortality with 95% CIs.
Table 2 shows results from the multivariable logistic regression analysis. When we conditioned the model on age only, influenza vaccination was associated with a 36% reduction in the odds of death among patients with COVID-19 (column 1, table 2). When we restricted our analysis to within-facility comparisons (column 2, table 2), the protective association was attenuated to 18% (adjusted OR (aOR) 0.82, 95% CI 0.77 to 0.88). The estimated associations changed only marginally when we further controlled for comorbidities and socioeconomic factors (columns 3 and 4, table 2), and when we excluded patients with COVID-19 where a positive laboratory SARS-CoV-2 test result was not documented in the electronic records (column 5, table 2). Obesity, pre-existing lung conditions, renal problems and neurological disorders were associated with higher mortality, with estimated ORs between 1.16 (respiratory conditions) and 1.35 (obesity). Patients suffering from asthma had marginally lower mortality odds (aOR 0.84, 95% CI 0.73 to 0.97) (column 5, table 2).
Estimated associations between influenza vaccination status and COVID-19-related mortality
Table 3 shows estimated associations between vaccination status and clinical care received. On average, influenza vaccination was associated with a 7% reduction in the odds of receiving intensive care (aOR 0.93, 95% CI 0.87 to 0.98), and a 17% reduction in the odds of receiving respiratory support (aOR 0.83, 95% CI 0.77 to 0.88). Online supplemental materials table 2 shows further details for all covariates included in this analysis.
Estimated associations between vaccination status and COVID-19 severity
Figure 2 shows estimated associations between vaccination status and COVID-19 mortality, stratified according to the documented timing of last influenza vaccine administration. As shown in online supplemental material figure S3, most of the vaccines (n=11 172, 90%) were received as part of the 2020 campaign, with 935 vaccinations (5.6%) administered after the self-reported onset of COVID-19 symptoms. In 11% of the patients (n=1127), influenza vaccine was administered before the 2020 campaign, mostly in 2019. As shown figure 2, panel A, we find protective effects for individuals whose last influenza vaccination was given in March 2020 or later, but not for individuals last vaccinated earlier or in 2019. Overall, influenza vaccines obtained as part of the 2020 campaigns were associated with 17% lower odds of mortality if the vaccine was given prior to the onset, and surprisingly with 36% lower odds of death if the vaccine was administered after onset of clinical COVID-19 symptoms—these two estimates are however not statistically different from each other.

{kind=link}
{kind=link}
Estimated association between influenza vaccination status and COVID-19 mortality dependent on timing of vaccine administration and stratified by patient age. Figure 2 compares COVID-19 mortality outcomes of non-vaccinated patients and of patients vaccinated against influenza at different time points. Estimates represent ORs based on multivariable logistic regression models with full set of covariates (95% CIs displayed as lines around the point estimate). The size of the grey squares is proportional to the sample size in each group. Panel A includes all patients; panels B and C include patients under and over the age of 60, respectively.
When we stratify our patients into two broad age groups (panels B and C, figure 2), we find larger protective effects for patients under the age of 60 years than for older patients when the vaccine was received prior to onset of symptoms (31% vs 12% lower odds). For vaccines given after onset of COVID-19 clinical symptoms, effect sizes in both age groups (under and above 60 years) were similar. No protective effects were found for either age group in cases when influenza vaccine was administered prior to the 2020 campaign. The full regression results underlying these figures are provided in online supplemental materials table 2.
Discussion
Here, we provide strong, and to our knowledge first patient-level evidence that people at risk of developing severe COVID-19 disease might benefit significantly from influenza vaccination. In the large and well-documented patient cohort from Brazil analyzed, we found that patients with COVID-19 who received the inactivated trivalent influenza vaccine in 2020—even if administered after the onset of SARS-CoV-2 infection-related clinical symptoms—had on average significantly higher chances of surviving and less need for intensive hospital care than patients without recent influenza vaccination. Patients obtaining an influenza vaccine differ potentially from non-vaccinated patients with respect to genetics, health status, health pursuing behaviour or other unknown biological or environmental factors that could at least partially explain the observed differences in clinical presentation and survival. We tried to address these concerns in multiple ways: (i) we restricted our comparisons to patients using the same health facility, which eliminates differences in healthcare access and quality of care; (ii) we controlled for self-reported race to address immunogenetic differences of populations and (iii) we controlled for age, gender and educational attainment to account for general differences in living conditions and health behaviours. Lastly, and most importantly, we controlled for an extensive set of pre-existing comorbidities documented in the medical records, which allows us to rule out any confounding through pre-existing health conditions. While we cannot rule out residual confounding through behavioural differences not manifested in acute or chronic health conditions (such as smoking or drinking behaviours), it seems somewhat unlikely that such confounders would fully explain the substantial protective effects observed in our large cohort.
The most immediate explanation for our observations is the prevention of potential influenza-SARS-CoV-2 coinfections.14 Although individual cases of such coinfections have been documented,15–17 larger studies have found this combination to be rather rare.18–20 Given that we found only 16 cases with such coinfections among the >50 000 patients in our cohort, we can mostly rule out coinfections as mechanism underlying the protective associations observed.
Influenza vaccines are designed to induce neutralising antibodies and virus-specific CD4+ and CD8+ T-cell responses.21 Influenza virus and SARS-CoV-2 display only limited nucleotide sequence similarity overall, and the induction of cross-neutralising antibodies and T-cells that directly target non-influenza viruses like SARS-CoV-2 seems unlikely.
A growing body of evidence shows that longer-lasting functional changes resembling memory can also be found in innate immune cells and tissue-resident stem cells.22 Trained innate immunity can be triggered by life vaccines,23 24 and result in well-known ‘off-target’ protection against a range of pathogens not directly targeted by the vaccine given.25 26 These protective effects have been shown to account for a significant share of the overall mortality reductions achieved by life vaccines.27 Inactivated influenza vaccination activates the innate immune system by triggering the toll-like receptor 7, resulting in an enhanced tumour necrosis factor-α and interleukin (IL)-6 production in peripheral blood leucocytes on antigen challenge and functional changes in the natural killer cell compartment lasting several weeks to months.28–34 The notion of beneficial effects of trained immunity induced by influenza vaccination35 appears consistent with the differential protective effects observed in the older (>60 years) versus younger (<60 years) COVID-19 patient group. Influenza vaccines are generally less effective in older than in younger individuals36; development of trained innate immunity thus also seems less likely among older patients.37
A surprising finding in our analysis is that influenza vaccination conducted at the time of onset of COVID-19 clinical symptoms or shortly thereafter was still associated with improved health outcomes. It is possible that the innate immune response induced by such late vaccination results in (i) more rapid and efficient SARS-CoV-2 clearance, preventing progressive dissemination into lower areas of lung tissues and/or (ii) dampening of the uncontrolled, destructive pro-inflammatory host response seen in COVID-19 at later, often fatal disease stages. In the absence of a COVID-19 vaccine and without a well-established, easily accessible treatment modality to control disease progression, induction of trained immunity exerting beneficial, ‘off-target’ effects might be an avenue for improving COVID-19 outcomes. Planned or ongoing clinical studies with BCG or repurposed live oral polio vaccine will help to understand these mechanisms better.38
Our study has several limitations. First, our study only focuses on hospitalised patients, and thus cannot directly assess the relationship between influenza vaccination and the likelihood of developing symptoms. A previous vaccination trial conducted in Hong Kong suggests that trivalent inactivated influenza vaccine can increase the risk of non-influenza viral infections among school-aged children,39 while a negative relationship between old age vaccination coverage and COVID-19 incidence was found at the county level in the USA.8 Second, our analysis is constrained by the data collected by the Brazilian government, which is somewhat limited, and does not include some potentially important factors such as other vaccines or smoking and drinking behaviours that may affect patient outcomes and that could potentially confound the analysis. Our data also do not contain any information on non-pharmaceutical interventions that may affect both the incidence and severity of COVID-19. It is also possible that clinicians decide to vaccinate only patients that are perceived to be in good health (and not vaccinate somebody already seriously ill)—this selection of healthier patients could potentially explain the effects observed, particularly in cases when patients are vaccinated after the onset of symptoms. The data set also contains only limited information on socioeconomic characteristics; while the main pathways of poverty (facility accessed and preconditions) are directly controlled for in our analysis, residual confounding through unobserved differences in living conditions is clearly possible. Our analysis is also subject to potential recall bias if some patients do not correctly recall the timing of their last vaccination and vaccination cards are not available. The data set also comes with a substantial amount of missing data on key variables. Information on vaccination status is available only for 45% of patients with COVID-19. Even though this missing data should not affect the internal validity of our study, it is not clear to what extent the empirical relationships observed in our sample will apply to the general Brazilian hospital population.
Despite these caveats, the incentives for governments and healthcare providers to promote influenza vaccination during the ongoing COVID-19 pandemic seem strong in light of the proven benefits of influenza vaccination to reduce influenza incidence.40 Older patients and patients with pre-existing health conditions like obesity, lung and renal diseases that have a higher odds of dying from COVID-19—as also shown here—might profit most from this intervention. Reducing the overall burden of respiratory viral infections during the influenza season will alleviate the work load of an already strained health work force, preserve care capacity for patients in greatest need and reduce the potential for nosocomial transmission of SARS-CoV-2 at treatment facilities.41
Supplemental material
Supplemental material
Data availability statement
Data are publicly available at the Brazilian Ministry of Health website.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
CD and AB are joint senior authors.
Contributors GF, AB, CD and NO-F conceptualised the paper. GF conducted the analysis and created a first draft. All coauthors provided input on the multiple draft versions and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Given that only publicly available and fully de-identified data were used in this research, the project does not classify as human subjects research.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.