Article Text

Abstract
Drug treatment to reduce cholesterol to new target levels is now recommended in four moderate- to high-risk patient populations: patients who have already sustained a cardiovascular event, adult diabetic patients, individuals with low density lipoprotein cholesterol levels ≥190 mg/dL and individuals with an estimated 10-year cardiovascular risk ≥7.5%. Achieving these cholesterol target levels did not confer any additional benefit in a review of 35 randomised controlled trials. Recommending cholesterol lowering treatment based on estimated cardiovascular risk fails to identify many high-risk patients and may lead to unnecessary treatment of low-risk individuals. The negative results of numerous cholesterol lowering randomised controlled trials call into question the validity of using low density lipoprotein cholesterol as a surrogate target for the prevention of cardiovascular disease.
- cardiovascular diseases
- cardiology
- public health
Statistics from Altmetric.com
Introduction
Millions of individuals worldwide are currently being treated with cholesterol lowering statin drugs based on the recommendations of the most recent guidelines on cholesterol management.1 2 The 2018 American Heart Association (AHA)/American College of Cardiology (ACC) cholesterol guidelines, like their European counterpart, are intended to reduce the risk of future cardiovascular disease by establishing targets for lowering low density lipoprotein cholesterol (LDL-C).1 2 Although this approach is supported by substantial evidence, it has never been validated. To test the validity of this paradigm, this analysis will critically review the clinical outcomes of randomised controlled trials (RCTs) of cholesterol reduction that did or did not meet these LDL-C targets.
Current recommendations
The 2018 AHA/ACC guidelines generally recommend LDL-C lowering drug therapy in the following moderate- and high-risk populations.
Moderate risk
Individuals aged 40–75 with diabetes and LDL-C between 70 and 189 mg/dL
Individuals aged 40–75 without atherosclerotic cardiovascular disease (ASCVD) or diabetes with LDL-C between 70 and 189 mg/dL and 10-year ASCVD risk ≥7.5% and <20%
High risk
Individuals with clinical ASCVD (secondary prevention)
Individuals with LDL-C ≥190 mg/dL
Individuals aged 40–75 without ASCVD or diabetes with LDL-C between 70 and 189 mg/dL and 10-year ASCVD risk ≥20%
For individuals at moderate risk, the guidelines recommend reducing LDL-C by 30% or more. For those at high risk, LDL-C should be reduced by 50% or more. The new guidelines recommend three classes of drugs for cholesterol reduction: β-Hydroxy β-methylglutaryl-CoA (HMG-CoA) reductase inhibitors (statins), cholesterol absorption inhibitors (ezetimibe) and proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9).
Randomised controlled trials
We performed a review of all RCTs of cholesterol reduction where the intervention was one of these three drug classes and the subjects matched one of the patient populations described above. Because our review involved three different drug classes and several different patient populations, we intentionally did not perform a meta-analysis. We initially identified relevant studies by searching Medline, PubMed and the Cochrane Central Register of Controlled Trials. We narrowed our search strategy by including relevant keywords (“statin”, “ezetimibe”, “PCSK9 inhibitor”, “low-density lipoprotein cholesterol”, “LDL-C”, “cholesterol”, “trial” and “randomised”) without restrictions on language or year of publication. We also reviewed the component RCTs in relevant meta-analyses of statins and PCSK9 inhibitors. We further refined our search by only selecting RCTs where the control group received either placebo or usual care, had a duration of ≥1 year, provided baseline characteristics that would enable calculation (where appropriate) of the 10-year ASCVD risk using the recommended Pooled Cohort Equations, described or allowed calculation of the percent change in LDL-C and reported cardiovascular events and/or mortality outcomes. When indicated, we also used risk enhancers and coronary artery calcium scores to better define risk as recommended in the guidelines.1 We assigned a quality score (A, B or C) to each study based on a combination of published recommendations for evaluating RCTs and the Cochrane risk of bias assessment tool.3 4 While the majority of these studies were of excellent quality and had a low overall risk of bias, we assigned a reduced quality score (B or C) to trials that had small population sizes (less than 1000 subjects), were not placebo controlled or had significant methodological or bias concerns. For each selected RCT we extracted the total mortality and combined cardiovascular event rates with the accompanying statistic for significance. If no clinical outcome statistic was reported, we calculated the odds ratio (OR) using the available data reported in the trial. Each trial was categorised as to whether it did or did not meet the LDL-C reduction target recommended in the AHA/ACC guidelines. We calculated both the number needed to treat (NNT) to prevent one cardiovascular event or death and the absolute risk reduction (the inverse of NNT) in each study that reported a statistically significant positive result. The 35 RCTs that met the above selection criteria are listed in tables 1 and 2.
Randomised controlled trials of cholesterol reduction in moderate-risk individuals (LDL-C reduction target ≥30%)
Randomised controlled trials of cholesterol reduction in high-risk individuals (LDL-C reduction target ≥50%)
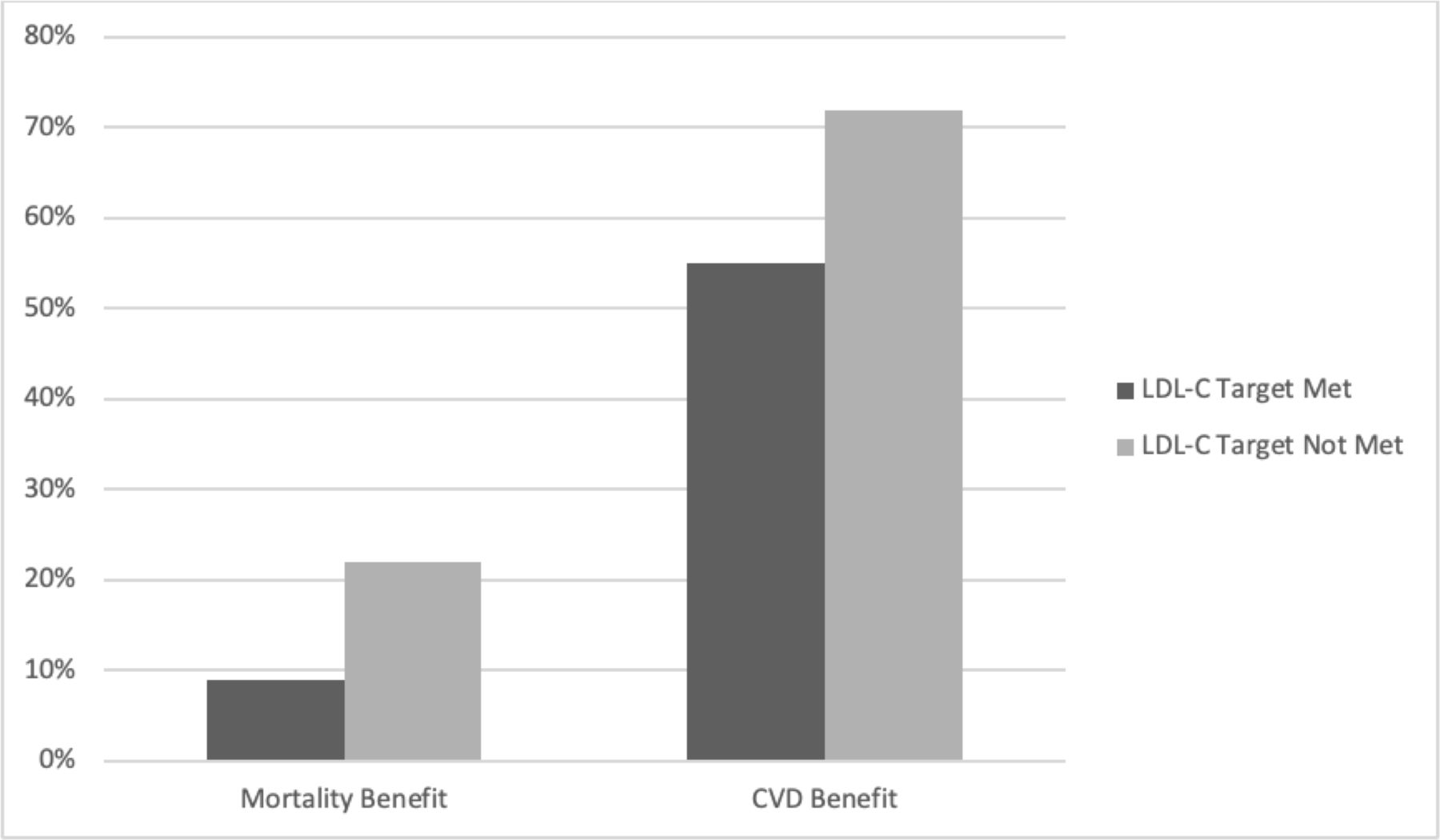
Of the 13 RCTs that met the LDL-C reduction target, only one reported a mortality benefit and five reported a reduction in cardiovascular events. Of the 22 RCTs that did not meet the LDL-C reduction target, four reported a mortality benefit and 14 reported a reduction in cardiovascular events (figure 1). Similar results were seen when analysing only higher quality studies (quality scores A and B, figure 2). The lack of consistent mortality and cardiovascular benefit was seen with all three drug classes. Although PCSK9 inhibitors are currently the most potent drugs for reducing LDL-C, it is not clear from this analysis whether or not this drug class is more likely to produce clinical benefit compared with statins or ezetimibe. In summary, mortality and cardiovascular benefit was more frequently reported in RCTs that did not meet the LDL-C targets than in those that did.
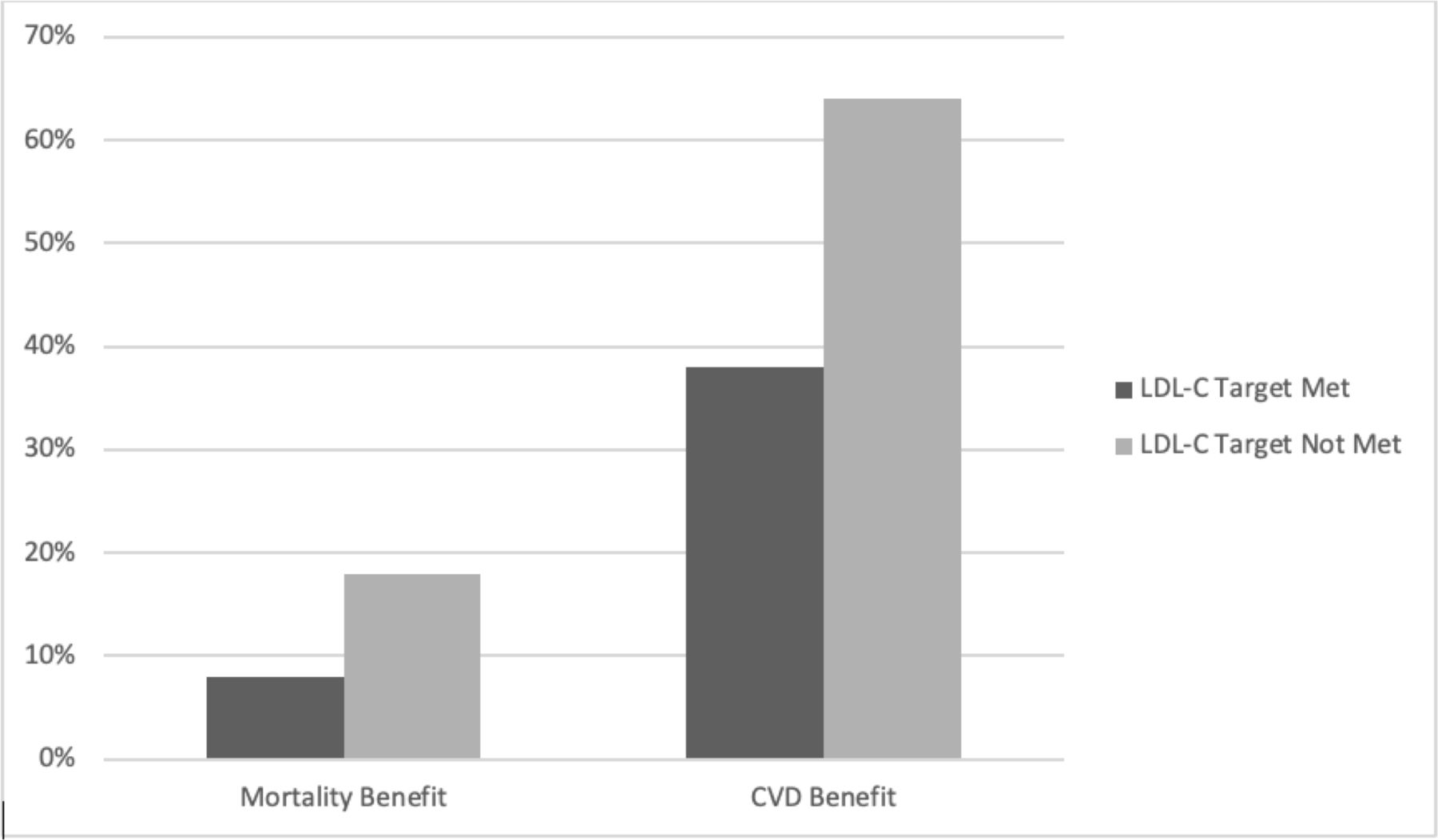
Per cent of low density lipoprotein cholesterol (LDL-C) lowering randomised controlled trials that reported benefit.

Per cent of higher quality low density lipoprotein cholesterol (LDL-C) lowering randomised controlled trials that reported benefit.
It is noteworthy that a beneficial reduction in cardiovascular events was seen with LDL-C reductions as little as 11%–15% in Aggressive Lipid-Lowering Initiation Abates New Cardiac Events (ALLIANCE) and Management of Elevated Cholesterol in the primary prevention Group of Adult Japanese (MEGA), while a lack of cardiovascular benefit was seen with LDL-C reductions as great as 50% or more in Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment With Alirocumab (ODYSSEY FH 1 and 2), Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) and Studies of PCSK9 Inhibition and the Reduction of Vascular Events (SPIRE 1 and 2).5–9 Similarly, the number needed to treat calculations show a discordance between the degree of LDL-C reduction and magnitude of benefit. For example, only 30 patients had to be treated with simvastatin for 5.4 years to prevent one death in the Scandinavian Simvastatin Survival Study (4S) trial whereas 250 patients required treatment with alirocumab (PCSK9 inhibitor) for 2.8 years to prevent one death in the ODYSSEY OUTCOMES trial (table 2).10 11 Yet, LDL-C was reduced by a mean of 35% in 4S compared with a mean LDL-C reduction of 55% in ODYSSEY OUTCOMES.
Limitations of this analysis
We have retrospectively analysed the results of 35 RCTs that were not intended for such an analysis. Some of these trials were not designed or powered to assess clinical outcomes and there is tremendous variability in patient populations, study durations, degrees of LDL-C reduction, the definition of a cardiovascular event endpoint and other potential confounding factors. Our selection criteria necessitated the exclusion of some important trials such as the PROspective Study of Pravastatin in the Elderly at Risk (PROSPER) due to a mean age of >75 years, the Heart Protection Study (HPS) because the percent change in LDL-C was not reported and could not be calculated, and Gruppo Italiano per lo Studio della Sopravvivenza nell'Insufficienza cardiaca-Heart Failure (GISSI-HF) because the 10-year risk of ASCVD could not be calculated.12–14 We included SPIRE 1 and 2, two RCTs that investigated bococizumag, a PCSK9 inhibitor, even though this drug will not be brought to market.9 The goal of reducing LDL-C by ≥30% or ≥50% in moderate- or high-risk individuals is based on the expected LDL-C reductions with moderate or high intensity statin therapy as described in the AHA/ACC guidelines.1 These LDL-C goals are comparable to those reported in the 2019 European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) cholesterol guidelines.2 We calculated the 10-year ASCVD risk using the Pooled Cohort Equations based on the mean or mode baseline characteristics of a theoretical trial subject who may or may not have relevance to an actual patient being considered for LDL-C lowering therapy.15 As emphasised in the AHA/ACC guidelines, lifestyle changes should be the primary intervention and decisions regarding LDL-C lowering drug therapy should be individualised and based on an informed discussion of the risks and benefits.1
Limitations of risk-guided targets
The risk-guided model matches the intensity of treatment to the ASCVD risk of the patient (eg, a high-risk patient warrants high-intensity LDL-C reduction). Ideally, this strategy should prevent cardiovascular events in patients at highest risk while avoiding unnecessary treatment in low-risk individuals. Unfortunately, the risk-guided model performs poorly in achieving these goals. Two separate studies retrospectively calculated risk scores (using risk calculators recommended at the time) in relatively young patients admitted to their respective hospitals with acute coronary syndromes or myocardial infarctions.16 17 Both studies reported that a majority of these patients would not have qualified for statin therapy based on their risk scores and then current cholesterol guidelines. Conversely, 44% of subjects in the Multi-Ethnic Study of Atherosclerosis (MESA) who were classified as statin candidates based on their risk scores were found to have zero coronary artery calcium scores, consistent with a very low risk of cardiovascular disease and potentially obviating the need for statin treatment.18
Limitations of LDL-C as a treatment target
Because of the putative role of LDL-C in the pathogenesis of ASCVD, it seems intuitive and logical to target LDL-C to prevent cardiovascular disease. Indeed, there is much evidence to support this approach. However, decades of RCTs of LDL-C reduction have failed to demonstrate a consistent benefit.19 Conspicuous by its absence in the AHA/ACC guidelines is any endorsement of niacin or cholesteryl ester transfer protein (CETP) inhibitors, agents with a proven track record of reducing LDL-C but failing to consistently save lives or prevent cardiovascular disease.20 21 To validate the theory that reducing LDL-C reduces the risk of cardiovascular disease (the lipid hypothesis), LDL-C lowering interventions must be efficacious. Considering that dozens of RCTs of LDL-C reduction have failed to demonstrate a consistent benefit, we should question the validity of this theory.22
Discussion
This analysis highlights the discordance between a well-researched clinical guideline written by experts and empirical evidence gleaned from dozens of clinical trials of cholesterol reduction. It further underscores the ongoing debate about lowering cholesterol in general and the use of statins in particular. In this analysis over three-quarters of the cholesterol lowering trials reported no mortality benefit and nearly half reported no cardiovascular benefit at all.
The widely held theory that there is a linear relationship between the degree of LDL-C reduction and the degree of cardiovascular risk reduction is undermined by the fact that some RCTs with very modest reductions of LDL-C reported cardiovascular benefits while others with much greater degrees of LDL-C reduction did not (MEGA, ALLIANCE, SEAS, ODYSSEY FH 1 and 2, SPIRE 1 and 2).5–9 23 This lack of exposure–response relationship is illustrated in figure 3, where the scatter plot and the calculated correlation coefficient (R) suggest there is no correlation between the percent reduction in LDL-C and the absolute risk reduction in cardiovascular events. Moreover, consider that the Minnesota Coronary Experiment, a 4-year long RCT that replaced saturated fat with vegetable oil rich in linoleic acid involving 9423 subjects, actually reported an increase in mortality and cardiovascular events despite a 13% reduction in total cholesterol.24 What is clear is the lack of clarity of these issues. In most fields of science the existence of contradictory evidence usually leads to a paradigm shift or modification of the theory in question, but in this case the contradictory evidence has been largely ignored simply because it doesn’t fit the prevailing paradigm.25 26

{kind=link}
{kind=link}
{kind=link}
Relationship between the per cent reduction in low density lipoprotein cholesterol (LDL-C) and the absolute risk reduction in cardiovascular events (R, correlation coefficient).
The results of all RCTs should be critically evaluated, in part because statistical conclusions can be misleading. For example, a New England Journal of Medicine editorial proclaimed that the IMPROVE-IT trial, a RCT of ezetimibe, provided proof that lowering LDL-C reduces the risk of coronary heart disease.27 28 This trial actually reported no mortality benefit of ezetimibe but did report a statistically significant reduction in combined cardiovascular events after a median follow-up of 6 years. Using the trial’s published data, we calculated that 56 subjects would need to be treated for 6 years to prevent one cardiovascular event (table 2). Stated another way, 55 out of 56 patients treated with ezetimibe for 6 years derived no apparent cardiovascular benefit even though their LDL-C levels were significantly reduced. This example illustrates how the number needed to treat calculation can be particularly helpful in assessing treatment effects in general and making informed decisions about cholesterol lowering interventions specifically.29
What to do now
Cardiovascular disease continues to be the leading cause of death worldwide. Between 2002 and 2013 statin use in the US nearly doubled, cholesterol levels are falling, yet cardiovascular deaths appear to be on the rise.30 31 In Sweden, recent widespread and increasing utilisation of statins did not correlate with any significant reduction in acute myocardial infarction or mortality, while in Belgium a very modest reduction in cardiovascular events was reported between 1999 and 2005, but primarily in elderly individuals not taking statins.32 33 These population studies suggest that, despite the widespread use of statins, there has been no accompanying decline in the risk of cardiovascular events or cardiovascular mortality. In fact, there is some evidence that statin usage may lead to unhealthy behaviours that may actually increase the risk of cardiovascular disease.34 35 The evidence presented in this analysis adds to the chorus that challenges our current approach to cardiovascular disease prevention through targeted reductions of LDL-C. Given the lack of clarity on how best to prevent cardiovascular disease, we encourage informed decision-making. Ideally, this includes a discussion of absolute risk reduction and/or number needed to treat at an individual patient level in addition to reviewing the potential benefits and harms of any intervention.
Ethics statements
Patient consent for publication
References
Footnotes
Correction notice This article has been corrected since it first appeared online. In the Discussion, the sentence "a 4-year long RCT of a low-fat diet" has been corrected to "a 4-year long RCT that replaced saturated fat with vegetable oil rich in linoleic acid". The term systematic review has been removed from this paper on three occassions. The term review is used instead.
Contributors The general thesis of this manuscript was conceived jointly. RDB was responsible for data collection, data verification and writing the initial draft. AM and MdL provided critical review and corrections to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note AM is a co-author of the ‘Pioppi Diet’ a lifestyle plan book that advocates for the benefits of a Mediterranean diet low In refined carbohydrates to to reduce heart disease risk and improve metabolic health. AM is also co-producer of documentary, The Big Fat Fix.