Article Text

Abstract
Objective: To compare the analgesic efficacy of single and multiple doses of ibuprofen with that of paracetamol in patients with knee or hip osteoarthritis (IPSO study).
Method: 222 patients were randomised in a double blind, multicentre study—156 (70%) had a painful knee joint and 66 (30%) a painful hip joint. The main efficacy criterion was pain intensity assessment after a single dose (ibuprofen 400 mg, paracetamol 1000 mg). Functional disability assessment and patient global assessment were carried out over 14 days.
Results: The sum of the pain intensity difference over 6 hours after the first administration was significantly higher (p = 0.046) in the ibuprofen group than in the paracetamol group. Over 14 days pain intensity decreased from the first day and was significantly lower in the ibuprofen group than in the paracetamol group (p<0.05). The functional disability of the patient was assessed using the WOMAC; the ibuprofen group improved significantly over 2 weeks compared with the paracetamol group for each of the subscales: stiffness (p<0.002), pain (p<0.001), physical function (p<0.002). The drugs were equally safe.
Conclusion: The IPSO study shows that for the treatment of osteoarthritic pain, ibuprofen 400 mg at a single and multiple dose (1200 mg/day) for 14 days is more effective than paracetamol, either as a single dose of 1000 mg or a multiple dose (3000 mg/day). Because ibuprofen and paracetamol have similar tolerability, this study indicates that the efficacy/tolerability ratio of ibuprofen is better than that of paracetamol in this indication over 14 days.
- AE, adverse event
- ANOVA, analysis of variance
- ITT, intention to treat
- NSAID, non-steroidal anti-inflammatory drug
- OA, osteoarthritis
- PI, pain intensity
- PID, pain intensity difference
- PP, per-protocol
- SPID, sum of pain intensity difference
- TOTPAR, total pain relief
- VAS, visual analogue scale
- WOMAC, Western Ontario and McMaster Osteoarthritis Index
- ibuprofen
- paracetamol
- pain
- efficacy
- osteoarthritis
Statistics from Altmetric.com
- AE, adverse event
- ANOVA, analysis of variance
- ITT, intention to treat
- NSAID, non-steroidal anti-inflammatory drug
- OA, osteoarthritis
- PI, pain intensity
- PID, pain intensity difference
- PP, per-protocol
- SPID, sum of pain intensity difference
- TOTPAR, total pain relief
- VAS, visual analogue scale
- WOMAC, Western Ontario and McMaster Osteoarthritis Index
The analgesic efficacy of ibuprofen given in low doses (up to 1200 mg/day) and paracetamol has been demonstrated in various painful conditions such as dental pain, sore throat, and dysmenorrhoea.1–,3 Osteoarthritis (OA) is the most common form of joint disease and is an important public health concern.4 It is a useful chronic pain model for assessing analgesic treatments.5 According to the “Recommendations for the registration of drugs used in the treatment of osteoarthritis” the recommended primary clinical end points in such assessments are pain assessment and functional disability.6 Ibuprofen and paracetamol were significantly more effective than placebo in placebo controlled studies in various pain conditions, ibuprofen 400 mg being more effective than paracetamol 1000 mg.2,7–,9 Paracetamol is the main reference level 1 analgesic currently used in clinical trials, especially in OA.10–,12 However, very few studies have compared the efficacy of paracetamol and ibuprofen in OA pain management. Bradley et al showed that ibuprofen at high doses (2400 mg/day) or at low doses (1200 mg/day) was at least as effective as paracetamol (4000 mg/day) in relieving pain in patients with OA of the knee over 4 weeks.10 More recently, a double blind study over 6 days found ibuprofen (1200 mg/day) at least as effective as paracetamol (4000 mg/day) in the treatment of pain from OA of the knee, and ibuprofen better than paracetamol in subjects with moderately severe or severe baseline pain.11 Both these studies involved repeated doses, but with no comparative data after a single dose. Apart from these two studies,10,11 there have been no efficacy studies conducted in OA of the pain relief achieved by both single and repeated doses of ibuprofen compared with paracetamol. The lack of clear evidence based on clinical trials was recognised by the published guidelines of the European League Against Rheumatism (EULAR) on OA of the knee.13
This study was therefore conducted in patients with knee or hip OA to compare the analgesic efficacy of ibuprofen with that of paracetamol after a single dose and a multiple dose over 14 days using the following main efficacy criteria: pain intensity assessment after a single dose (ibuprofen 400 mg, paracetamol 1000 mg) and a functional disability assessment and patient global assessment over 14 days (ibuprofen 400 mg, paracetamol 1000 mg, each three times daily).
PATIENTS AND METHODS
Patients
Thirty one general practitioners included patients of either sex, ages 50–85 years, with chronic pain (score at least 50 mm on a 100 mm visual analogue scale (VAS)) due to confirmed knee or hip OA and requiring analgesic treatment for 2 weeks.
Two or three visits were conducted for each patient depending on whether a washout period was needed. A washout period of up to 3 days was required if non-steroidal anti-inflammatory drugs (NSAIDs) and/or analgesics had been taken within 72 hours and 8 hours respectively of the pre-inclusion visit. In the washout period patients were given a rescue drug (paracetamol, 500 mg tablets, up to six tablets daily) to be used in case of real need and a diary card to record doses taken; these patients attended the inclusion visit after the washout period. Patients who did not require a washout period completed the inclusion visit directly after the pre-inclusion visit. Patients with painful OA of the lower limbs (femorotibial or femoropatellar OA of the knee or OA of the hip) diagnosed according to the clinical and radiological criteria (x ray examination performed within the previous year) from the American College of Rheumatology classification were included.14–,16
The main non-inclusion criteria were any serious respiratory, hepatic, or renal failure, prosthesis of the affected joint or surgery of the affected joint within the previous 3 months or planned within the next 3 months, a known hypersensitivity to any NSAID or paracetamol, need for anti-inflammatory treatment, having a hydrarthrosis requiring a puncture, and use of oral corticosteroids within the previous 8 days.
Study design
The IPSO study (ibuprofen, paracetamol study in OA) was a randomised, multicentre, double blind, parallel group comparative study. Before the start of the study the protocol was approved by the Committee for Protection of Persons Participating in Biomedical Research (Hospital Ambroise Paré, Boulogne Billancourt, France). The study was conducted according to good clinical practices and the Declaration of Helsinki (October 1996). All patients provided written informed consent before participating in the study.
Patients were given the study drug to start the day after enrolment for 14 days of treatment. All the assessments concerned the affected joint, defined as the reference joint by the investigator at the inclusion visit. During the treatment period the patient completed a daily diary card to assess the spontaneous pain intensity and pain relief after the first intake of the study drug. The average daily pain intensity was assessed from the first to the 13th day of treatment. A global assessment of efficacy was made by the patient at the final visit.
The functional disability was assessed by the patients and reported by the investigators at the inclusion and final visits. The WOMAC (Western Ontario and McMaster Osteoarthritis Index) was used as a disease-specific measure.16–,18
Any adverse event occurring during the study period was also recorded by the patients.
Study drug
Patients meeting the selection criteria (after a washout period if needed) were randomly assigned to one of the treatment groups. To ensure double blind conditions, the study used matching encapsulated ibuprofen and paracetamol tablets (Creapharm, Bordeaux, France). Patients received capsules of either ibuprofen 200 mg or of paracetamol 500 mg. The drug was self administered and patients were instructed to take two capsules three times daily for 14 days.
Evaluation of efficacy
The primary efficacy outcome measure was based on the patients’ assessment of pain intensity every hour over 6 hours after the first administration of treatment, on a 100 mm VAS.2,16 The sum of pain intensity difference (SPID) was calculated from the pain intensity difference (PID).
All the secondary outcomes measures and other variables were determined either related to the first or repeated administrations as follows.
Assessment related to the first administration over the first 6 hours of treatment: the pain intensity (PI), the PID, and the peak PID were calculated based on the 100 mm VAS with end points of “no pain” and “very intense pain”. Pain relief was recorded, using a numeric scale (end points 0% relief to 100% relief, in blocks of 10%) and the total pain relief (TOTPAR) was calculated.2
Assessment related to repeated administration each evening from the inclusion visit to the thirteenth day of treatment: the average intensity of the daily pain (PI) was assessed by the patient using a four point verbal scale (none, mild, moderate, severe).
Assessment related to repeated administration at the end of the study: the global efficacy of the treatment was assessed by the patient using a four point verbal scale (no efficacy, poor efficacy, good efficacy, very good efficacy). The sleep quality was assessed using a four point verbal scale (very bad, bad, good, very good).
The functional disability was assessed using the WOMAC and consisted of 24 validated items grouped into three categories: stiffness (2 questions), pain (5 questions), and physical function (17 questions) evaluated using five point scales (from 0 = none to 4 = very severe).16–,18 The results were added to obtain the WOMAC total score. The results for the different subscales and the total score were normalised to 0–100 (good to bad).
Evaluation of safety
All adverse events (AEs) during the study were collected from the patients’ diary cards and from the investigators’ reports in the case report form and classified according to the description, duration, severity, frequency, and outcome. Investigators assessed the relationship between AEs and the study drug. AEs were classified using the Coding Symbol Thesaurus for Adverse Reaction Terms (COSTART).19
Statistical methods
Because there were no previous data on pain intensity evaluation using a VAS in OA, the sample size was evaluated based on data from two previous studies which had used ibuprofen for treatment of pain associated with other diseases. It was calculated that a sample size of 196 patients (98 patients in each group) was needed to detect a difference of 8 mm (measured on a VAS) in the pain intensity between ibuprofen and paracetamol, after a single dose, under the assumption of an risk of 5%, and a standard deviation of 20 mm.2,8 A total of 200 patients had to be randomised to ensure at least 98 patients in each group in the intention to treat (ITT) population, defined as all randomised patients who had taken at least one dose of the study drug and had had at least one evaluation of efficacy.
The initial characteristics of the two treatment groups were described for the ITT population: frequency and percentage for the qualitative variables; mean, standard deviation, median and range for the quantitative variables. The changes between the initial and final visits on physical examination (normal/abnormal), in vital signs, weight, and height were compared between the two groups using Student’s t test. All variables were summarised by descriptive statistics at each visit and by groups. All statistical tests were two sided and performed at the 5% significance level.
For the primary criteria, the differences between the two treatment groups in SPID after the first administration and the daily average PI over the 14 days of treatment were analysed by an analysis of variance (ANOVA: Student’s t test) in the ITT population.
For all the secondary efficacy end points, analysis was performed on the ITT population, using ANOVA with repeated measurements and Student’s t test or a Wilcoxon test when necessary.
The WOMAC was analysed for the three subscales and for the total score. The difference in scores between baseline and after treatment in both groups was determined and the mean change was compared using a Wilcoxon test.16,17
The per-protocol population (PP) was defined as all ITT subjects without a major protocol deviation which might have affected the evaluation of efficacy.
The safety population was defined as all randomised patients who received at least one dose of the study drug.
RESULTS
Study group
Two hundred and twenty two patients were randomised to the ibuprofen or the paracetamol group. All took at least one dose of the study drug and had one evaluation of efficacy and so were included in the ITT population and safety population. Baseline characteristics were similar in the two groups (table 1⇓). Patients in both treatment groups had had arthritis for about 4.5 years. Sixty six (30%) patients had a painful hip joint and 156 (70%) patients had a painful knee joint, the femorotibial joint being mainly affected. All patients had a baseline pain intensity >50 mm as described on a VAS (mean (SD) 71.7 (10.7) mm).
Study groups—baseline characteristics
Seven (3%) patients required a washout period—four in the ibuprofen group and three in the paracetamol group. The mean (SD) treatment duration was 13.8 (1.3) days—the same for both groups (13.9 (1.3) days in the ibuprofen group and 13.8 (1.3) days in the paracetamol group).
For the primary outcome analysis, five patients were excluded from the randomised population because of missing data (either baseline evaluation or more than one evaluation) (fig 1⇓). Thirty three patients were excluded from the PP population because of major protocol deviations (fig 1⇓). Exclusion was mainly because pain assessment values were not available or missing (n = 21), and/or a second intake of treatment had been taken before the end of the first 6 hours’ assessment (n = 8), and/or treatment had started before the first evaluation (n = 5), and/or a forbidden drug had been taken (n = 2).

Disposition of the patients. *Patients excluded because of missing values for pain assessment on VAS scale: 3 in the ibuprofen group, 2 in the paracetamol group; †patients excluded because pain assessment values were not available or missing (9 in the ibuprofen group, 12 in the paracetamol group), a second drug intake started before the end of the first 6 hours (3 in the ibuprofen group, 5 in the paracetamol group), study treatment started before the first pain evaluation (4 in the ibuprofen group, 1 in the paracetamol group), forbidden concomitant treatment started (2 in the ibuprofen group); some patients had more than one reason.
Treatment discontinuation
The study was completed by 212 (95%) patients (108 in the ibuprofen group and 104 in the paracetamol group). Ten (5%) patients withdrew early from the study (4 owing to recovery (2 in each group), 2 because of lack of efficacy in the paracetamol group, 3 because of AEs (1 in the ibuprofen group, 2 in the paracetamol group), and 1 owing to both lack of efficacy and AEs in the paracetamol group).
Primary outcome
The SPID over 6 hours after the first administration of study treatment was significantly higher (p = 0.046) in the ibuprofen group than in the paracetamol group in the ITT population (table 2⇓). The PP population gave similar results (mean (SD) SPID −94.5 (119.6) in the ibuprofen group, −66.5 (88.7) in the paracetamol group, p = 0.069).
Sum of pain intensity difference (SPID) over 6 hours in the ITT population
Secondary outcomes
Efficacy
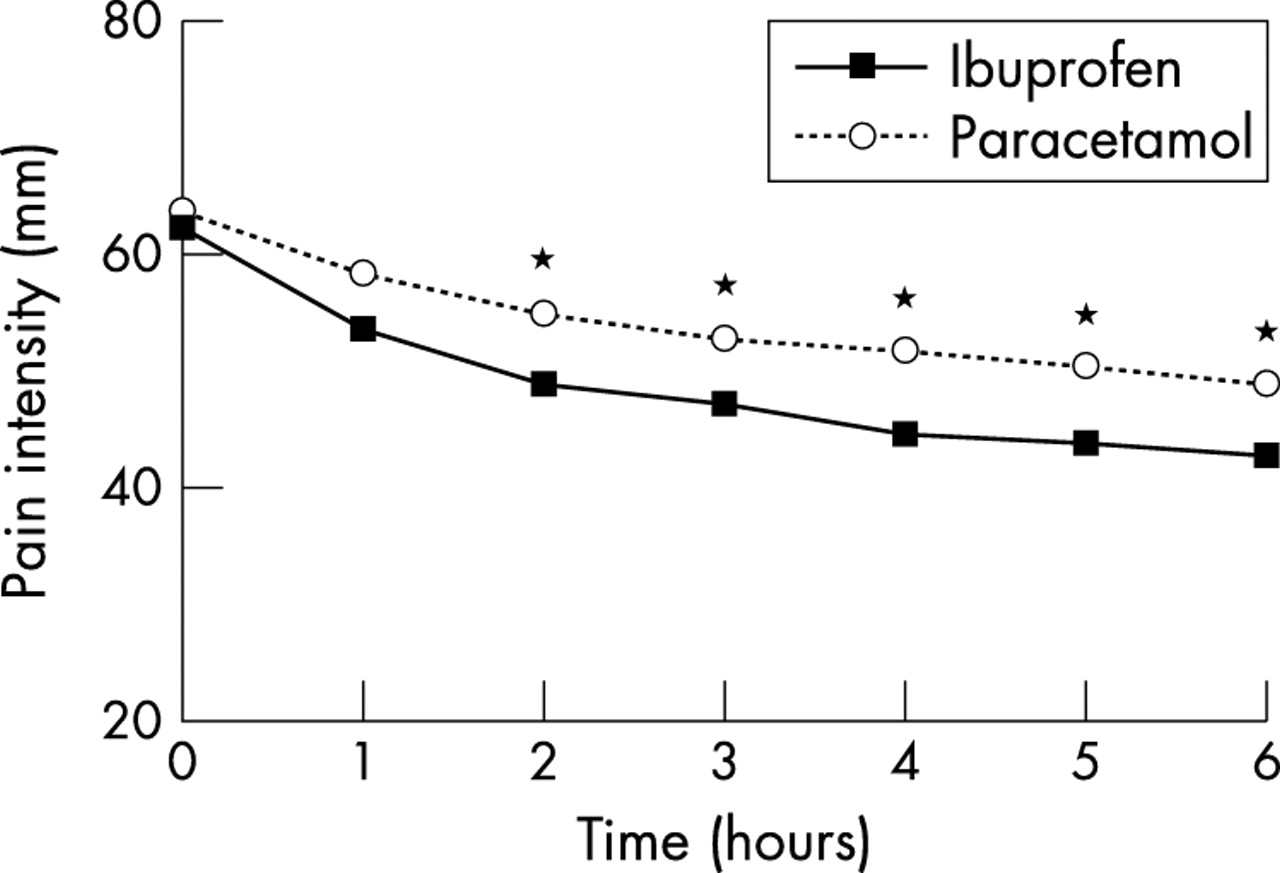
The mean (SD) peak pain intensity difference as measured by the VAS after a single dose was higher in the ibuprofen group (−27.6 (19.6)) than in the paracetamol group (−21.2 (17.2)), with a significant difference between the groups (p = 0.011). Figure 2⇓ shows that there was a significant difference favouring ibuprofen between the groups from the second to the sixth hour (p⩽0.042) on the evolution of the pain intensity in the first 6 hours. The pain intensity difference increased from the first to the sixth hour, with a significant difference in favour of ibuprofen between the groups (p = 0.046). The mean (SD) TOTPAR over 6 hours was significantly higher in the ibuprofen group (234.8 (150.1)) than in the paracetamol group (189.5 (136.5), p = 0.02). The treatment effect was also evaluated for the affected joint (knee or hip). The ANOVA with interaction of treatment and joint was not significant (SPID, p = 0.289; TOTPAR, p = 0.354) and showed that the effect of treatment was independent of the type of joint.

Evolution of the pain intensity during 6 hours after the first dose. *p<0.05, Student’s t test.
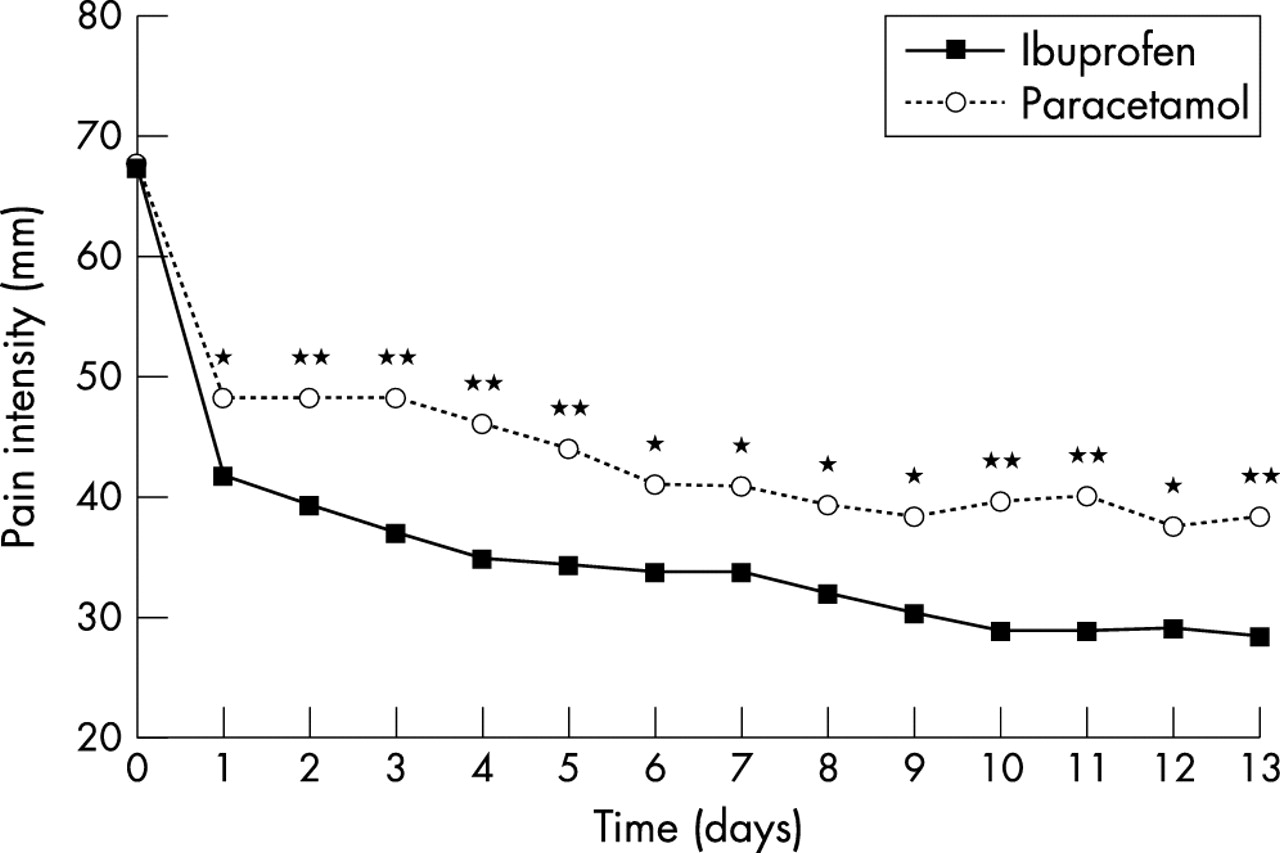
The improvement of pain was also analysed after repeated doses over 14 days of treatment. Figure 3⇓ shows that pain intensity assessed by a VAS decreased from the first day of treatment and was lower in the ibuprofen group than in the paracetamol group (p<0.05). The average pain intensity was also assessed by a four point verbal scale. These results confirmed those obtained by the VAS, with an improvement of pain intensity for both treatments (fig 4⇓), but with a significant difference in favour of ibuprofen (p<0.001).

Evolution of the pain intensity over 14 days of treatment assessed by a VAS. *p<0.05; **p<0.005, Student’s t test.

Evolution of the pain intensity during 14 days of treatment assessed by a four point verbal scale. Ibuprofen versus paracetamol: p<0.001, Wilcoxon test.
The sleep quality assessed on a four point scale before treatment started and at the end of the study improved for both treatments, with no significant difference between the groups (data not shown).
Stiffness, pain, and physical function were analysed after repeated doses to assess the functional disability of the patients. As indicated by their responses on the WOMAC, the ibuprofen group had significantly less pain (p<0.001) and significantly improved stiffness (p = 0.002) and physical function (p = 0.002) compared with the paracetamol group after 2 weeks of treatment (table 3⇓). The total WOMAC score was improved for both treatments with a statistically significant difference in favour of ibuprofen (table 3⇓).
WOMAC subscales
More patients reported a good to very good global efficacy in the ibuprofen group (67.5%) than in the paracetamol group (37.8%) (p = 0.001) (fig 5⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Global efficacy assessment at the end of the study using a four point verbal scale. Ibuprofen versus paracetamol: p = 0.001, Wilcoxon test.
Safety
A total of 51 (23%) patients reported at least one AE during the treatment and with no significant difference between the treatment groups: 26/111 (23.4%) in the ibuprofen group and 25 (22.5%) in the paracetamol group. No serious AE was reported. The most common AEs belong to the two COSTART systems: body as a whole system for 20 patients and digestive system for 24 patients (table 4⇓). The total number of patients with gastrointestinal events (abdominal pain and digestive system combined) was similar for the two treatment groups: 17 in the ibuprofen group and 16 in the paracetamol group. The AEs most frequently reported were nausea, abdominal pain, dyspepsia, and dizziness (table 4⇓). Only three AEs were severe (2 asthenia, 1 pain); all the others were of mild to moderate intensity, with no statistically significant difference between the groups.
Adverse events
One patient in the ibuprofen group (with moderate dyspepsia) and three patients in the paracetamol group (with moderate myalgia, mild constipation, and mild varicose veins) discontinued the treatment owing to AEs.
DISCUSSION
The IPSO study clearly shows that a significant and a more marked reduction in pain was experienced by patients with OA of the hip or knee with ibuprofen 400 mg than with paracetamol 1000 mg, both in the 6 hours after the first single dose of treatment and during the 14 days of multiple doses (1200 mg/day for ibuprofen, 3000 mg/day for paracetamol).
Several studies have shown that ibuprofen and paracetamol are efficacious in the management of patients with OA.10,11,20–,25 To study pain relief it is interesting to assess the immediate analgesic effect after the first dose of analgesic treatment using criteria such as a VAS or a numerical pain scale. After the first administration of the study drug, over the first 6 hours the SPID was significantly higher in the ibuprofen group than in the paracetamol group (p = 0.046, ITT population). Our results show a more marked significant reduction in pain with ibuprofen than with paracetamol.
All the secondary efficacy criteria led to the same conclusion. The total pain relief over 6 hours was significantly higher in the ibuprofen group than in the paracetamol group (p = 0.02): ibuprofen provided nearly 23% more pain relief than paracetamol as measured by the numerical scale. During the first 6 hours, a significant difference (p = 0.042) between the groups was seen for the pain intensity hourly from 2 hours, indicating an earlier efficacy response with ibuprofen. The PID significantly increased every hour from 1 hour to 6 hours, with a significant difference between the groups (p = 0.046) in favour of ibuprofen. These results consistently confirm that ibuprofen (400 mg) is more efficacious than paracetamol (1000 mg) in the 6 hours after the first dose is taken. The treatment effect was the same whether the hip or the knee was affected. To our knowledge this study is the first to compare the efficacy of single doses of ibuprofen and paracetamol in the treatment of OA pain.
Because OA is primarily a chronic disease, studies must also focus on repeated administration. Efficacy was also compared over 14 days’ administration using the maximum ibuprofen or paracetamol doses approved in France at the time of the study for the management of mild to moderate pain, although the paracetamol maximum dose has since been increased to 4000 mg daily for more severe pain. The better efficacy of ibuprofen compared with paracetamol was confirmed every day over 14 days.
For repeated administration it is interesting to assess the functional states with a measure like the WOMAC, which is commonly used in OA-specific states based on patient self assessment of physical function, stiffness, and pain.17,26 The efficacy analysis using the WOMAC indicated a significant improvement over 2 weeks in favour of ibuprofen for each of the subscales: stiffness (p<0.002), pain (p<0.001), and physical function (p<0.002) and also for the total score (p⩽0.001). Use of the WOMAC enabled this study to evaluate improvement not only in pain but also in stiffness and physical function; the results were consistent with the conventional pain assessment scales, with a significantly greater improvement in the mobility of the patients with OA with ibuprofen than with paracetamol. Clearly, the greater beneficial effect of ibuprofen on stiffness and functional disability was linked to the better pain relief achieved with ibuprofen throughout the 14 day study. These results further confirm the usefulness of the WOMAC in demonstrating efficacy in clinical drug trials, as first shown by Bellamy et al17 and confirmed more recently by Davies et al.26
Only two studies have compared ibuprofen with paracetamol in OA pain management. In a double blind comparison of the efficacy of paracetamol up to 4000 mg daily with that of an analgesic dose of ibuprofen (1200 mg daily) or an anti-inflammatory dose (2400 mg daily)10 the Stanford Health Assessment Questionnaire disability and pain scales27 were expanded and used to evaluate pain at rest, pain on walking, and walking distance after 4 weeks of treatment. There was no evidence of better efficacy in the three treatment groups except for rest pain, which decreased more markedly in both ibuprofen groups than in the paracetamol group. In a further analysis of that study, the improvement detected by the treatments in the reduction of disability and rest pain was not necessarily dependent on an anti-inflammatory effect such as that expected with ibuprofen 2400 mg/day.28 Yet another reanalysis of that study to determine whether greater pain intensity at the start of the treatment could predict a better response to treatment29 found that a higher level of pain at the time treatment was initiated predicted a quantitatively greater decrease in pain, but that this was true whatever the treatment used.
These results10,28,29 contrast with those of a later double blind study11 in patients with knee OA with moderately severe or severe baseline pain, which showed that ibuprofen 1200 mg/day was statistically significantly better than paracetamol 4000 mg/day after 4 and 6 days of treatment. The results of the IPSO study confirm and extend those data, with a significant difference between ibuprofen and paracetamol each day over 14 days.
The better efficacy of ibuprofen shown in the present study, as well as in the study by Altman,11 is also confirmed by two recent surveys.30,31
Because the prevalence of OA increases significantly with age, safety needs special consideration.32 A large scale study, the PAIN study33 showed that the tolerability of ibuprofen given at over the counter doses (up to 1200 mg daily) for 6 days was equivalent to that of paracetamol and better than that of aspirin for a variety of mild to moderate pain conditions. Moreover, analysis of comparative tolerability in patients with specific musculoskeletal conditions in the PAIN study reached the same conclusion.34 Doyle et al showed that placebo treated and ibuprofen treated (1200 mg daily) patients had a similar incidence of gastrointestinal AEs during 10 days’ treatment.35 In our study, safety was satisfactory for both treatment groups.
Pain is a matter of public health concern. Patients with OA need pain relief as well as functional disability improvement for a short and long term period. The present study demonstrated the superior clinical efficacy of ibuprofen over paracetamol in the treatment of pain in knee or hip OA at a single dose and over 14 days. Paracetamol is the initial drug recommended for systemic treatment of symptomatic OA of the hip and knee by the American College of Rheumatology.36,37 It was therefore the most appropriate drug to use for comparison with ibuprofen in an efficacy and safety study of OA pain control. Further treatment recommendations will have to take into account the present data, linked to the better efficacy/tolerability ratio of ibuprofen compared with paracetamol, to elaborate a more widely based treatment strategy for OA pain.
Acknowledgments
The authors thank the investigators for their involvement in the clinical trial.
The study was funded by Boots Healthcare France.