Article Text

Abstract
Background: Currently, there is no consistent evidence that breast feeding reduces the risk for sudden infant death syndrome (SIDS). Arousal from sleep is believed to be an important survival mechanism that may be impaired in victims of SIDS. Previously it has been shown that arousability is impaired by the major risk factors for SIDS such as prone sleeping and maternal smoking.
Aims: To establish whether arousability was altered by method of feeding, and whether breast fed infants would have lower arousal thresholds.
Methods: Forty three healthy term infants were studied using daytime polysomnography on three occasions: 2–4 weeks post-term, 2–3 months post-term, and 5–6 months post-term. Multiple measurements of arousal threshold (cm H2O) in response to nasal air jet stimulation applied alternately to the nares were made in both active sleep (AS) and quiet sleep (QS) while infants slept supine. Arousal thresholds and sleep period lengths were compared between formula fed and breast fed infants at each age.
Results: Arousal thresholds were not different between breast fed and formula fed infants in QS. However, in AS breast fed infants were significantly more arousable than formula fed infants at 2–3 months of age. There was no difference between groups of infants when sleep period length was compared at any study.
Conclusions: Breast fed infants are more easily aroused from AS at 2–3 months of age than formula fed infants. This age coincides with the peak incidence of SIDS.
- breastfeeding
- arousal
- sleep
- sudden infant death syndrome
- AS, active sleep
- QS, quiet sleep
- SIDS, sudden infant death syndrome
Statistics from Altmetric.com
Despite the dramatic decline in the incidence of sudden infant death syndrome (SIDS) following worldwide education programmes to encourage supine sleeping, prevention of overheating, and protection from both maternal and passive smoke exposure,1–4 SIDS still remains the major cause of death in infants between the ages of 1 month and 1 year.5,6 Arousal from sleep is believed to be an important survival mechanism that may be impaired in victims of SIDS.7 In support of this idea, a prospective study found fewer body movements and fewer arousals from sleep in infants who subsequently died from SIDS, than in control infants.8
Although many studies have shown benefits of breast feeding for infant health, there is no consistent evidence that it reduces the risk for SIDS. Retrospective case-control studies in the USA,9 New Zealand,10 and more recently from Scandinavia11 have found that breast feeding appeared to be protective for SIDS—that is, fewer SIDS than control infants were breast fed. The cessation of breast feeding was also earlier in the SIDS cases than in the controls.10 However, in other smaller studies, after adjusting for confounding factors, breast feeding was not associated with any significantly altered risk for SIDS.12–14 In the much larger CESDI SUDI study carried out in the United Kingdom between 1993 and 1996, breast feeding also did not alter the risk for SIDS when confounding factors had been accounted for.15 Thus SIDS organisations, although promoting breast feeding in their SIDS reduction campaigns, have not been able to support the idea that breast feeding is protective of SIDS.
Previously we and others have shown that evoked arousability from sleep is impaired by the major risk factors for SIDS, namely prone sleeping,16–21 maternal smoking,22–24 prematurity,25 and recent infection.26 In this study we wished to examine whether arousability was altered in sleeping infants by method of feeding, and hypothesised that breast fed infants would have lower arousal thresholds.
METHODS
Subjects
Ethical approval for this project was granted by the Monash Medical Centre Human Ethics Committee. All subjects were volunteers recruited from the maternity wards and Jessie McPherson Private Hospital, Monash Medical Centre, Melbourne. Written informed consent was obtained from parent(s) prior to commencement of the study. Forty three infants (24 females, 19 males) were studied between September 1997 and October 2001. All infants were born at term between 38 and 42 weeks gestation (mean 39.8 (SEM 0.2) weeks), with normal birth weights (mean 3534 (63) g, range 2700–4725 g). Apgar scores were 3–10 (median 9) at 1 min and 6–10 (median 9) at 5 min. Infants were studied on three occasions: study 1 (n = 42): 2–4 weeks after birth (mean age 18 (1) days, range 8–32 days); study 2 (n = 39): 2–3 months post-term (mean age 73 (1) days, range 63–84 days); and study 3 (n = 36): 5–6 months post-term (mean age 173 (2) days, range 155–213 days).
Infants were divided into two groups at each study according to their method of feeding (table 1). Breast fed infants received no more than one feed of formula per day (n = 2 at study 3), and formula fed infants were exclusively formula fed. All infants were receiving solids at the 5–6 month study. One infant did not complete study 1, two infants withdrew from the project after the first study, one infant was unavailable for study 2 (but completed studies 1 and 3), and four infants did not complete study 3.
Demographics of breast fed and formula fed infants at arousal studies
Recording methods
Daytime polysomnography recordings were made from all infants between 10:00 and 16:00. Electrodes for recording physiological variables were attached to the baby while it fed and, when drowsy, the infant was placed supine in a bassinet under dim lighting and constant room temperature (22–23°C). The study did not begin until the infant was in a stable sleep state. Recordings were made on a polygraph (model 78A 16-channel recorder, Grass Instrument Company, Quincey, MA, USA) of electroencephalogram (EEG), electro-oculogram (EOG), submental electromyogram (EMG), and electrocardiogram (ECG), instantaneous heart rate (HR), thoracic and abdominal breathing movements (Resp-ez Piezo-electric sensor, EPM Systems, Midlothian VA, USA), expired CO2 (CO2/O2 analyser, Engstrom Eliza MC, Bromma, Sweden), blood oxygen saturation (SpO2) (Biox 3700e Pulse Oximeter, Ohmeda, Louisville, CO, USA), and abdominal skin temperature (YSI 400 series thermistor (NTC) probes). Sleep state was assessed as either QS, AS, or indeterminate sleep using EEG, behavioural, heart rate, and breathing pattern criteria.27
Stimulus and arousal criteria
A pulsatile air jet (frequency 3 Hz for 5 s) delivered to the nostrils of the infant was used to induce arousal in both AS and QS. Multiple measurements of arousal threshold across each sleep state were calculated according to an established protocol.16,17,22,25,26 Briefly, the stimulus was presented alternately to the left and right nostrils; if the infant failed to arouse, the air jet pressure was increased when the stimulus was again presented to that nostril. Whenever an arousal response occurred the pressure was decreased. The changes of pressure between each presentation ranged from 25 to 100 cm H2O, but were usually 100 cm H2O. The maximum pressure setting was 950 cm H2O. Arousal threshold was calculated as the mean stimulus driving pressure between each arousal and non-arousal response. The four criteria used to define arousal were: a change in ventilation pattern of more than two breaths, an observed behavioural response, an HR acceleration of greater than 10% above baseline, and an increase in submental EMG activity. All of these changes needed to occur within 7 s of the stimulus onset, allowing for the time delay to reach peak HR acceleration. For each physiological variable, the 10 s of recording immediately preceding the stimulus presentation provided the baseline level used to assess the change in that variable. Previously we have shown that our stimulus evokes arousal significantly more often (p<0.001) than spontaneously occurring arousal measured during stimulus calibration preceding each stimulus presentation using the same arousal criteria.16,17,22,25,26
Data analysis
Data were first tested using the Kolmogorov-Smirnov normality test and the Levene median test for equal variance. Arousal thresholds for left and right nostrils were compared using a one way analysis of variance (ANOVA, SigmaStat v2, SPSS Inc.). No difference between arousal thresholds was found between nostrils in either position; accordingly, the data for each nostril have been pooled for all subsequent analyses of arousal threshold. Mean arousal thresholds for AS and QS were calculated for each infant and compared within individual studies between breast fed and formula fed infants and between male and female infants at each study with non-paired Student’s t test. The lengths of sleep periods were determined for complete periods of both AS and QS, and those periods terminated by arousals induced by our stimuli were excluded from analysis. Sleep cycle length was determined as the time between the onset of successive periods of AS and only complete periods of AS and QS were included in this analysis. Mean sleep period length and sleep cycle length were compared between groups with non-paired Student’s t test. All values are expressed as mean (SEM) and a p value of <0.05 was considered significant.
RESULTS
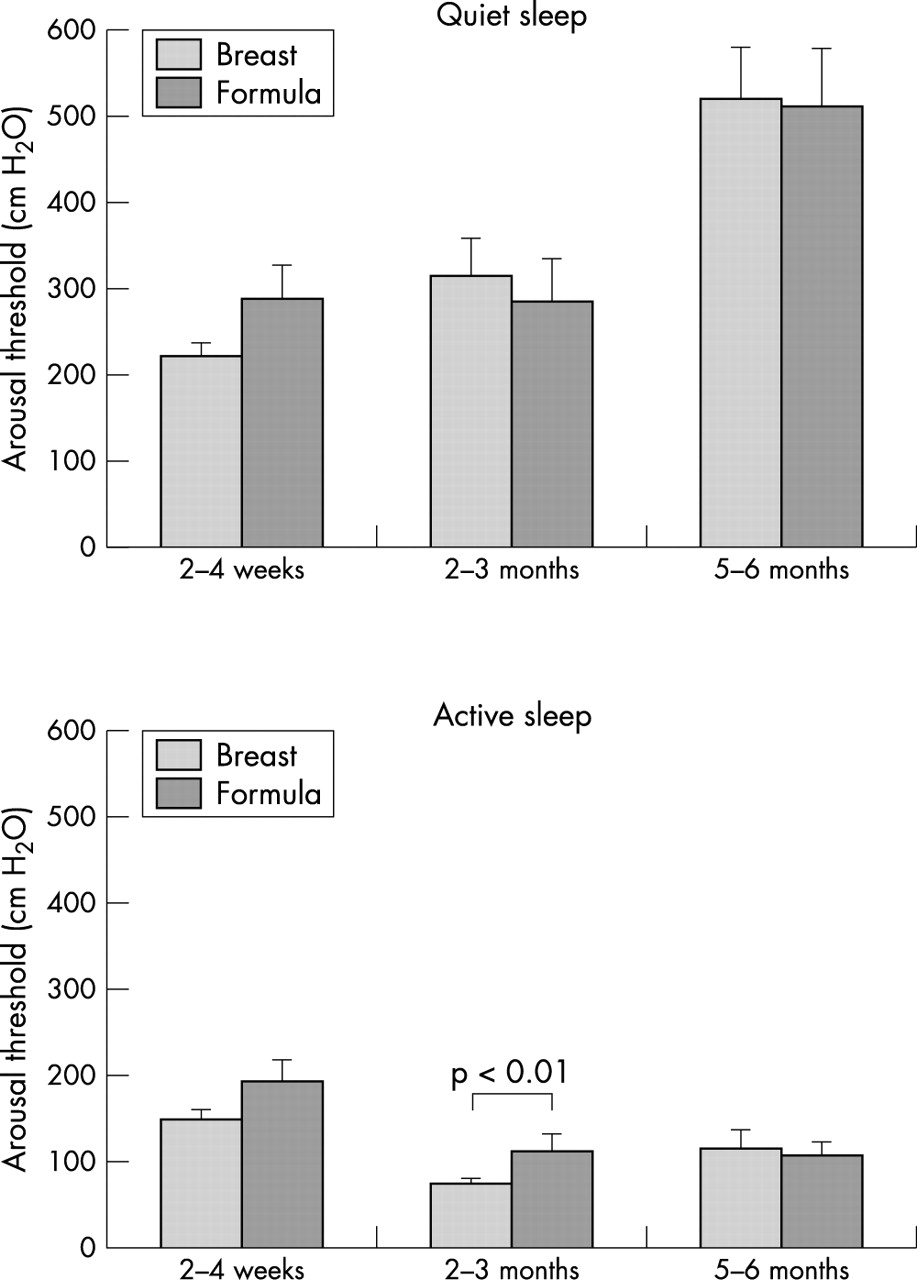
There was no significant difference between the two groups in either infant age or weight at any of the three ages studied (table 1). Arousal thresholds were not different between breast fed and formula fed infants in QS at any of the three ages studied. However, in AS breast fed infants were significantly more arousable (that is, had lower arousal thresholds) than formula fed infants at 2–3 months of age (p<0.01) (fig 1).
{kind=link}
Arousal thresholds in quiet sleep and active sleep of breast fed and formula fed infants.
Arousal thresholds were significantly increased in QS compared to AS in both groups of infants at all three ages studied (p<0.001), with the exception of the formula fed group at 2–4 weeks of age.
When males and females were compared, there were no significant differences in arousability in either sleep state at any of the three ages studied (table 2).
Effects of sex on arousal thresholds (n = number of infants)
There was no difference between breast fed and formula fed infants when sleep period length was compared at any study (table 3). However, at 5–6 months of age breast fed infants had significantly longer sleep cycles (p<0.01).
Sleep period and sleep cycle times (min) in breast fed and formula fed infants
DISCUSSION
In this study we have shown that breast fed infants are more easily aroused from AS at 2–3 months of age than formula fed infants. This age coincides with the peak incidence of SIDS, and method of feeding had no influence on arousability at either 2–3 weeks or 5–6 months of age when the incidence of SIDS is reduced.9 Differences in sleeping patterns between the two groups could not explain these findings.
In previous epidemiological studies there have been inconsistent findings on the protective effects of breast feeding for SIDS, with some studies showing a protective effect9–11 while others did not show this.12–15 Currently, it is hypothesised that SIDS may result from a deficit in arousal responses to a life threatening event such as a prolonged respiratory pause, bradycardia, or hypotension.28,29 In support of this, the major risk factors for SIDS, prone sleeping and maternal smoking, have been shown to decrease arousability from sleep.16–24 In contrast, sucking on a pacifier (or dummy) which has been shown to be a protective factor for SIDS30–32 has also been shown to increase arousability.33
Previous studies by our group and others have consistently shown that arousal from sleep occurs at lower thresholds in AS compared with QS.16,17,19,22,25,26,34–36 The present study also found this sleep state effect on arousability. In recent studies from our group examining arousal responses to a mild hypoxic stimulus we found a similar sleep state difference. Importantly however these studies also showed that, while infants frequently failed to arouse to 5 minutes of hypoxia (15% O2) in QS, they always aroused in AS.37 Thus arousal from AS may be of vital importance in a life threatening situation.
It has been suggested that formula feeding may be a marker for other risk factors for SIDS such as prematurity and low maternal education or maternal smoking.12 In the present study, all infants studied were term born and mothers were from a wide range of secondary and tertiary education levels. Approximately half (n = 20) of the study group mothers reported smoking during pregnancy and after birth. At the first study 16 of these infants were in the breast fed group and four in the formula fed group; because of these small numbers it was not possible to analyse the effects of maternal smoking in this study.
Postmortem studies have shown that formula fed infants dying from SIDS have significantly lower levels of docosahexaenoic acid (DHA) in the frontal lobes of their brains than do breast fed infants. This long chain fatty acid is concentrated in neural tissue and has been reported as a predictor of developmental indices at 1 year of age in preterm infants.38,39 In support of this, a recent study of newborn term infants has shown that higher concentrations of maternal DHA were associated with a more mature pattern of infant sleep.40 In addition, breast fed infants have been shown to have better visual evoked potential acuity than formula fed infants, which may also be a result of improved neuronal function.41 Infants dying of SIDS have been reported to have altered or less mature autonomic function.42,43 Any delay in neuronal maturation could affect the arousal pathway and hence alter arousability.
We did not show a difference in sleeping pattern between breast fed and formula fed infants. In a previous study by our group we showed that arousal threshold in active sleep were unaffected by the length of the AS period with infants always being readily arousable. In QS however, arousal thresholds increased with time spent asleep.44 Previous studies examining the sleep/wake patterns of breast fed and formula fed infants have shown conflicting results. A study of term infants showed that breast fed infants studied between 2 weeks and 4 months slept longer than formula fed infants, and in addition formula fed infants cried more frequently in the evenings and at night.45 In contrast, a study of premature infants in the newborn nursery at 4–6 weeks postnatal age showed that breast fed infants spent more time crying (around one hour per day) than did formula fed infants.46 Our studies were carried out during the day and we did not record total time asleep and awake because if infants awoke and cried they were immediately consoled.
Numerous epidemiological studies have shown an increased risk for SIDS in male infants.3 However, our study did not detect any difference in arousability between male and female infants. Previous studies have however identified that male infants slept for shorter periods of time at night and developed a sleeping rhythm later than female infants,47,48 suggesting that male infants may be more arousable.
In conclusion, our study has provided evidence that breast fed infants are more readily aroused from AS than formula fed infants at the age when SIDS risk is greatest. This study supports breast feeding of infants during the critical risk period for SIDS (2–4 months) as reduced arousal, particularly in AS, could impair the ability of an infant to respond appropriately to a life threatening situation.
Acknowledgments
The authors wish to thank the staff of the maternity wards at the Monash Medical Centre and Jessie McPherson Private Hospital and the parents and infants who participated in this study. We thank Professor Richard Harding, Department of Physiology, Monash University for his comments on the manuscript.
REFERENCES
Footnotes
-
This project was supported by SIDSaustralia, Sudden Infant Death Research Foundation of South Australia, and SIDassist
Linked Articles
- Atoms