Article Text

Abstract
Aims: To identify subgroups of children with otitis media with effusion (OME) that might benefit more than others from treatment with ventilation tubes.
Methods: An individual patient data (IPD) meta-analysis on seven randomised controlled trials (n = 1234 children in all), focusing on interactions between treatment and baseline characteristics—hearing level (HL), history of acute otitis media, common colds, attending day-care, gender, age, socioeconomic status, siblings, season, passive smoking, and history of breast feeding. Outcome measures that could be studied were mean time spent with effusion (n = 557), mean hearing levels (n = 557 in studies that randomised children, and n = 180 in studies that randomised ears), and language development (n = 381).
Results: In the trials that treated both ears the only significant interaction was between day-care and surgery, occurring where mean hearing level was the outcome measure. None of the other baseline variables showed an interaction effect with treatment that would justify subgrouping. In the trials that treated only one ear, the baseline hearing level showed a significant but not pervasive interaction with treatment—that is, only with a cut-off of 25 dB HL.
Conclusions: The effects of conventional ventilation tubes in children studied so far are small and limited in duration. Observation (watchful waiting) therefore seems to be an adequate management strategy for most children with OME. Ventilation tubes might be used in young children that grow up in an environment with a high infection load (for example, children attending day-care), or in older children with a hearing level of 25 dB HL or greater in both ears persisting for at least 12 weeks.
- HL, hearing level
- IPD, individual patient data
- OME, otitis media with effusion
- RCT, randomised controlled trial
- VT, ventilation tube
- WW, watchful waiting
- IPD meta-analysis
- otitis media with effusion
- ventilation tubes
- hearing
- language
- grommets
Statistics from Altmetric.com
- HL, hearing level
- IPD, individual patient data
- OME, otitis media with effusion
- RCT, randomised controlled trial
- VT, ventilation tube
- WW, watchful waiting
In most western countries the insertion of conventional ventilation tubes is the most common operation in children. The main indication for the procedure in young children is persistent otitis media with effusion (OME), which refers to an accumulation of fluid in the middle ear cavity behind an intact tympanic membrane without the signs and symptoms of an acute infection. The functional effect of OME is a conductive hearing loss, which has been thought to result in impairments of speech, language, and cognitive development.1,2 The aim of the insertion of ventilation tubes is to restore hearing to normal levels and to prevent developmental problems.
Several randomised controlled trials (RCTs) have been performed to study the effectiveness of treatment with ventilation tubes. Most examined the effect on hearing and reported only short term improvements.3–7 Four trials also studied the effect on language development; one of these found a marginal effect of ventilation tubes on language development;8 the other three studies did not show a clear effect.9–11
Several trials in OME, however, do suggest that specific subgroups might benefit more from treatment with ventilation tubes than others. For example, two trials suggested a possible interaction effect between hearing loss at baseline and treatment—that is, children with a greater hearing loss at baseline appeared to benefit more from treatment with ventilation tubes than children with a smaller hearing loss.3,11,12 The power of these trials was, however, too small to perform valid and reliable subgroup analyses. The best way to address criteria for targeting interventions is to do larger trials. However, it is cost effective to performing an individual patient data (IPD) meta-analysis to make the most efficient use of data that already exist.
An IPD meta-analysis is a meta-analysis on the individual original data of performed trials; this is specifically useful for studying the interactions necessary for subgroup analysis, because it provides the necessary power and precision.13–15 Furthermore, IPD meta-analyses offer other advantages as compared with a meta-analysis of the published literature. These advantages include better standardisation of case definitions, outcomes, and covariates; the ability to fully test the assumptions of heterogeneity; better control of confounding; consistent categorisation of subpopulations; and assessment of sampling bias. IPD meta-analysis requires international collaborations, which in turn help to reach consensus on what new trial information is required, and to prospectively update the meta-analyses and synthesise new information on outcomes.16,17 We were able to establish such an international network and collected, validated, and reanalysed data on the effect of ventilation tubes in randomised patients with OME included in seven randomised trials.
METHODS
Selection of the trials
A systematic literature search was performed from PUBMED, the proceedings of the international symposia on recent advances in otitis media, and the Cochrane Library. Details of the search strategy can be found on the ADC website. To be selected for the IPD meta-analysis, trials had to be randomised to a high standard. Trials had to include children aged 0–12 years of age with tympanometrically and/or otoscopically confirmed persistent bilateral OME, and the comparison had to be between short term ventilation tubes (VT) and watchful waiting (WW). The primary investigators of all selected trials were asked for the raw data of their trials. Trials that treated one ear and used the contralateral ear in the comparison instead of a concurrent control group were analysed separately.3,4,7
Data collection and endpoints
The obtained data were thoroughly checked18 for consistency, plausibility, and integrity of randomisation and follow up. Any queries were resolved by the responsible trial investigator or statistician.
Primary outcome measures were mean time spent with effusion (measured by tympanometry), hearing (measured by pure-tone audiometry or age related hearing assessment), and language development (measured by Reynell test*). Calculation of the mean time spent with effusion was based on an interpolation from type B tympanograms during the follow up visits. If a child had OME at two successive measurements, the days between these measurements were counted as days with effusion. If a child had OME at the first measurement but not at the second (or vice versa), only half of the days were counted as days with effusion. Hearing level was expressed as a mean hearing loss (if possible averaged over 500, 1000, 2000, and 4000 Hz) measured where possible by air conduction, pure tone audiometry. In trials that randomised children rather than ears the binaural average was taken. Reynell language scores were expressed as standardised z scores. As the language development was measured at different follow up times in two of the trials included, we had to assume that the mean scores at 6 and 9 months follow up could be aggregated, as well as the means at 12 and 18 months follow up. The trials that studied behaviour and quality of life used differing outcome measures, so pooling was not possible.
Effect modifiers (subgroups) that could be included in the IPD were: hearing level at baseline (n = 744), history of acute otitis media (yes/no; n = 616), upper respiratory infections (yes/no; n = 619), attending day-care (yes/no; n = 625), gender (boys/girls; n = 651), age (n = 651), socioeconomic status (educational level of mother; n = 632), siblings (yes/no; n = 634), season (winter, spring, summer, autumn; n = 650), history of breast feeding (yes/no; 464), and parental smoking (yes/no; 466). All these modifiers were measured prior to randomisation.
Analyses and statistics
In the first instance, all analyses were performed as randomised (so called “intention-to-treat” principle). Differences in mean time spent with effusion, mean hearing loss, and language development between both treatment groups were tested with the Student’s t test for independent groups.
Second, a prognostic model was made to study predictors of poor outcome, which was defined as a score worse than the median hearing loss, time with effusion, and language development. Subsequently, the individual predictors were used to study possible effect modification—that is, the effects of ventilation tubes within subgroups of patients. Fixed effect regression analyses were performed with treatment group, the potential effect modifier, a dummy for the particular study, and an interaction term (treatment group × potential effect modifier) as independent variables, and hearing loss, time spent with effusion, and language development as dependent variables.
Separate analyses were performed for the trials that treated both ears, and the trials that treated only one ear. As the pathogenesis of otitis media is known to be multifactorial,19 children with more than one predisposing factor might have more persistent or severe disease and hence might benefit more from treatment with ventilation tubes than children with only one such factor. To study this possibility, we also studied the combinations of predictors found in the multivariate prognostic models.
Finally, to address therapeutic efficacy rather than intervention policy (and acknowledging that ventilation tubes were inserted for short term use), the children in whom ventilation tubes were in situ and functioning were compared with children without or with non-functioning tubes (for example, according to the “as treated principle”).
RESULTS
The literature search identified 15 randomised trials that compared the insertion of short term ventilation tubes with watchful waiting in children with persistent OME. Five trials were excluded from the meta-analyses due to inadequate randomisation (k = 2),20,21 or because all children had undergone adenoidectomy (k = 3).22–24 Seven triallists placed their data at the first author’s (MR) disposal.3,4,7,8,10,11,25 The data of the other three trials were not available.5,6,9 Of the seven available trials, four trials8,10,11,25 treated both ears (n = 801) with either ventilation tubes or watchful waiting, whereas the other three trials3,4,7 treated only one ear and used the contralateral ear as the comparison (n = 433) (see also fig 1). Table 1 presents the main characteristics of the seven included trials.
Characteristics of the seven trials included in the IPD meta-analyses
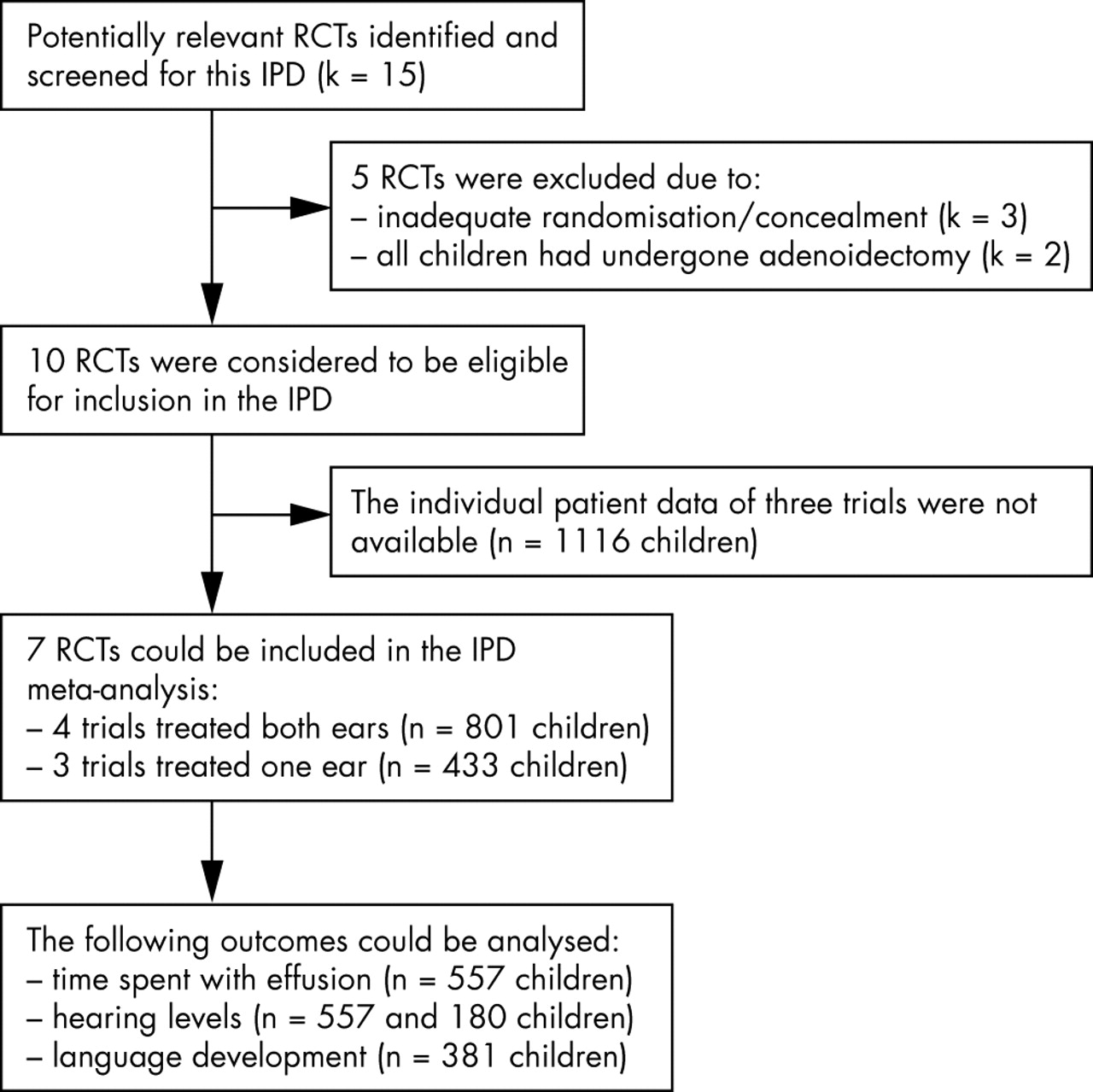
QUOROM flow chart.
Trials that randomised children
The mean time spent with effusion could be studied in 557 children. During a follow up period of 12 months, the mean time spent with effusion was 19.7 weeks (95% CI 17.6 to 21.9) in the children treated with ventilation tubes and 37 weeks (95% CI 34.9 to 39.1) in the watchful waiting group (p = 0.0001). The mean hearing level could be studied in 574 children. At 6 months follow up the mean hearing level in children treated with ventilation tubes was 26.6 dB HL (SE 1.0) compared to 31.1 dB HL (SE 1.0) in the watchful waiting group (p = 0.001). At 12 and 18 months follow up, no differences were found (table 2). The language development could be studied in 381 children. No differences were found in children treated with ventilation tubes and the children in the watchful waiting group at 6–9 and 12–18 months follow up (p = 0.09 and p = 0.19, respectively) (table 3). However, in one of the trials,8 85% of children in the WW group had received surgery by 18 months postoperative; such a high rate of transfer to “active treatment” severely limits the ability to draw a conclusion of an effect.
Mean binaural hearing levels during follow up in trials (k = 4) that randomised children (pooled effect estimate)
Mean language development (standardised z score) during follow up (k = 3 trials)
Univariate predictors of poor hearing at 6, 12, and 18 months follow up were baseline hearing loss, age, season, attending a day-care centre, and being breast fed. However, the analyses of interaction by fixed effect regression showed that with hearing as outcome measure, ventilation tubes were only differentially effective in children attending day-care (fig 2). The mean hearing level in children attending day-care treated with ventilation tubes was 7 dB HL better compared to children attending day-care that were randomised to the watchful waiting group after 6 months follow up, whereas a difference of only 0.9 dB HL was found in the children not attending day-care (p = 0.02 for interaction). For the other possible subgroups no differences were found.

(A) Stratified results regarding the interaction between day-care and treatment (k = 4 trials) after 6 months follow up. p = 0.02 for interaction. Number of cases in each subgroup: VT and day-care, n = 123; WW + day-care, n = 118; VT without day-care, n = 67; WW without day-care, n = 63. (B) Stratified results regarding the interaction between day-care and treatment (k = 4 trials) after 12 months follow up. p = 0.61 for interaction. Number of cases in each subgroup: VT and day-care, n = 127; WW + day-care, n = 112; VT without day-care, n = 68; WW without day-care, n = 61.
Univariate predictors of poor language development were baseline hearing loss, attending a day-care centre, age, and season. Ventilation tubes were, however, not differently effective in children with greater versus smaller hearing loss at baseline, breast versus bottle fed children, children randomised in summer versus winter, children attending day-care versus those not attending day-care, and older versus younger children.
Univariate predictors for mean time spent with effusion were attending a day-care centre, gender, and season, but again no interactions justifying subgrouping were found.
Children with more than one risk factor appeared to benefit slightly more from treatment with ventilation tubes, but the accumulation was only weak, like most of the individual risk factors.
In the efficacy (as treated) analysis, large significant effects on hearing level were found between children with functioning ventilation tubes and children without or with non-functioning tubes. The mean hearing level in children treated with functioning tubes was about 6 dB HL better compared to children with non-functioning tubes, both after 6 and 12 months follow up (p = 0.0001) However, also in this analysis no significant interaction effects indicating relevant subgroups were found.
Trials that randomised ears
In the three trials that only treated one ear and used the contralateral ear as the comparison, only baseline hearing level, age, and gender could be studied as possible indicators, and mean hearing level was the only measured outcome. Other variables and/or outcomes were not measured, or the data were so heterogeneous that they could not be pooled. Furthermore, only cases in which a ventilation tube was inserted in one ear and in whom the contralateral ear was used as the control ear (n = 160) were included in the analysis—that is, children who also had undergone adenoidectomy were excluded in the analysis. The studies were also on older children that were almost all at school. In these trials ventilation tubes did appear to be differentially effective in the ears with a worse baseline hearing level. However, if the hearing level at baseline was dichotomised at various cut-off values, only a cut-off of 25 dB HL showed an effect. After 6 months follow up, ears treated with ventilation tubes and a baseline hearing loss of 25 dB HL or greater improved 10 dB HL more than ears with a similar baseline hearing loss but which were not treated with ventilation tubes. The ears of children treated with ventilation tubes and a baseline hearing loss smaller than 25 dB HL improved only 4 dB HL more than the control ears (p = 0.05 for interaction) (fig 3A). After 12 months follow up, ears treated with ventilation tubes and a baseline hearing loss of 25 dB HL or greater improved 7 dB HL more than ears with a similar baseline hearing loss but which were not treated with ventilation tubes. The ears of children treated with ventilation tubes and a baseline hearing loss smaller than 25 dB HL improved only 3 dB HL more than the control ears (p = 0.28 for interaction) (fig 3B).

{kind=link}
{kind=link}
{kind=link}
(A) Stratified results regarding the interaction between baseline hearing level and treatment in the trials that randomised ears (k = 3) after 6 months follow up. p = 0.05 for interaction. Number of cases in each subgroup: VT and ⩽25 dB HL, n = 60; WW and ⩽25 dB HL, n = 57; VT and >25 dB HL, n = 20; WW and >25 dB HL, n = 23. (B) Stratified results regarding the interaction between baseline hearing level and treatment in the trials that randomised ears (k = 3) after 12 months follow up. p = 0.28 for interaction. Number of cases in each subgroup: VT and ⩽25 dB HL, n = 58; WW and ⩽25 dB HL, n = 55; VT and >25 dB HL, n = 20; WW and >25 dB HL, n = 23.
DISCUSSION
The pooled results of meta-analysable studies confirm that treatment with short term ventilation tubes produces limited hearing improvement of only short duration—that is, only as long as the tubes are in situ and patent. Children aged 3 years or younger attending day-care and children aged 4 years or older with a hearing level of 25 dB HL or greater in both ears persisting for at least 12 weeks might benefit more from treatment with such ventilation tubes. Baseline hearing level, however, did not emerge as a clear selection criterion in the way suggested by current guidelines and by prevailing professional belief—that is, average hearing level at baseline did not obviously modify the effect estimate.
Interaction results for baseline hearing level with treatment differed between the trials that randomised children and trials that randomised ears. This difference is probably due to four factors. The first is the control for individual variance achieved by analysing treatment effects within subjects, reducing measurement error. The second is that there was no switching in the trials that randomised ears, whereas in the trials that randomised children, 11–85% of the children in the WW group received ventilation tubes during follow up. The third is the distribution of the mean hearing loss at baseline. In the trials that treated only one ear, the range of the mean hearing loss at baseline was 7.5–47.5 dB HL, whereas the range in the trials that treated both ears was 17.5–60 dB HL. Consequently, the power of the subgroup analysis with a cut-off around 25 dB HL was larger in the trials that treated one ear. Furthermore, the results suggest that children with a more definite hearing loss have been included in the more recently performed randomised trials—that is, the trials that randomised children. This follows from the trend in guidelines that suggest inserting ventilation tubes only in children with persistent OME and a hearing loss ⩾20 dB HL. However, even for children with marked hearing loss at baseline, treatment with ventilation tubes was only effective in the short term—that is, as long as the tubes are in situ and patent. It has to be considered whether the absence of interaction between treatment and baseline hearing is due to insensitive outcome measurement. Hearing level, however, is unusually precise as an outcome measure.
The interaction effect that distinguishes children according to day-care attendance might be explained by the infection load in day-care. The infection load in day-care may result in an increased risk of new episodes with effusion. Consequently, children attending day-care and who are not treated with ventilation tubes might suffer from more frequent or longer hearing losses over a longer period. However, if this hypothesis was true, one would also expect an interaction effect for AOM, upper respiratory tract infections, season, and number of siblings, or for a composite of all these, which was not found. The day-care interaction effect therefore needs to be studied further in young children.
In the current analyses only European trials could be included. A question could be raised whether the expected benefits for VT for subgroups would be more evident in US data. The main-effect results of individual trials performed in the USA are very similar to those in the included trials—that is, ventilation tubes had a beneficial effect on hearing in the short term, but this effect disappeared in the long term.5,6,26 Paradise et al, for instance recently showed that prompt insertion of ventilation tubes in children with otitis media did not measurably improve developmental outcome in under 3 year olds.9 It is therefore not to be expected that inclusion of data from the trials performed in the USA would have changed the results of the meta-analysis.
Subgroups that might benefit more from treatment with ventilation tubes include those with speech or language delays, behaviour and learning problems, Down’s syndrome, or children with cleft palate. These could not be studied in this IPD meta-analysis as these subgroups were excluded in the individual trials. The experience of many clinicians that these subgroups of children benefit more from treatment with ventilation tubes has not yet been evidenced in RCTs. As the question whether to treat these children with ventilation tubes is very relevant for clinical practice, future trials studying these specific subgroups are justified.
Prospective cohort studies have shown that OME during early life may influence later language development negatively,27,28 whereas others failed to find such an association.29,30 These findings suggest that OME may not be an innocent disease that should be left untreated. The insertion of tubes can, on the other hand, lead to adverse effects such as tympanosclerosis, atrophy, and retraction.31,32
In conclusion, the benefits of short term ventilation tubes in children studied so far are small and related to the continued presence and patency of the tubes. Therefore an initial period of watchful waiting seems to be the appropriate management strategy for most children with OME. None of the baseline variables showed a strong interaction effect with treatment justifying subgrouping. If ventilation tubes are used, they could be inserted in young children growing up in an environment with a high infection load (for example, children attending day-care) or in older children with a hearing level of 25 dB or greater in both ears persisting for at least 12 weeks. As no evidence is yet available for the subgroups of children with speech/language delays, behaviour and learning problems, and/or syndromes, the clinician will need to make his/her own decision regarding treatment for such children.
What is already known on this topic
-
Trials performed so far have shown no or only marginal effects on hearing and language development
-
The insertion of ventilation tubes is, however, still the most common operation in children in western countries
What this study adds
-
Observation seems to be an adequate management strategy for most children with OME
-
Ventilation tubes might be used in young children that grow up in an environment with a high infection load (for example, children attending day-care), or in older children with a hearing level of 25 dB HL or greater in both ears, persisting for at least 12 weeks
REFERENCES
Supplementary materials
The supplement is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Search strategy
Footnotes
-
↵* A standardised and validated test measuring the comprehensive language development.
-
Funding: this study was funded by a grant from the Dutch Health Care Insurance Board (VAZ01121)
-
Competing interests: none declared