Article Text

Abstract
Objective To systematically review current evidence regarding the minimum acceptable risk reduction of a cardiovascular event that patients feel would justify daily intake of a preventive medication.
Methods We used the Web of Science to track the forward and backward citations of a set of five key articles until 15 November 2016. Studies were eligible if they quantitatively assessed the minimum acceptable benefit—in absolute values—of a cardiovascular disease preventive medication among a sample of the general population and required participants to choose if they would consider taking the medication.
Results Of 341 studies screened, we included 22, involving a total of 17 751 participants: 6 studied prolongation of life (POL), 12 studied absolute risk reduction (ARR) and 14 studied number needed to treat (NNT) as measures of risk reduction communicated to the patients. In studies framed using POL, 39%–54% (average: 48%) of participants would consider taking a medication if it prolonged life by <8 months and 56%–73% (average: 64%) if it prolonged life by ≥8 months. In studies framed using ARR, 42%–72% (average: 54%) of participants would consider taking a medication that reduces their 5-year cardiovascular disease (CVD) risk by <3% and 50%–89% (average: 77%) would consider taking a medication that reduces their 5-year CVD risk by ≥3%. In studies framed using 5-year NNT, 31%–81% (average: 60%) of participants would consider taking a medication with an NNT of >30 and 46%–87% (average: 71%) with an NNT of ≤30.
Conclusions Many patients require a substantial risk reduction before they consider taking a daily medication worthwhile, even when the medication is described as being side effect free and costless.
- Cardiovascular Diseases
- Communication
- Decision-making
- Risk Assessment
- Guideline
Statistics from Altmetric.com
Introduction
Cardiovascular disease (CVD) is the leading cause of premature death and reduced disability adjusted life-years worldwide.1 2 Thus, CVD prevention, which may require the initiation of lifelong medication aiming at modifying specific risk factors of future adverse events,3 has been, and will continue to be, a public health priority.
Clinical practice guidelines (CPGs) were developed to assist practitioners and patients in their decisions about appropriate healthcare interventions. However, disease preventive guidelines face a crucial challenge: individuals at risk often feel healthy and might perceive medications as unnecessary, particularly those having uncertain benefits and/or unpleasant side effects. This challenge can lead to disagreement between how guidelines panel and patients value the benefits and harms of preventive medications.4 For instance, while guidelines panels may assume that the benefits of a preventive intervention outweigh any potential harm, individual patients may not agree with their trade-off. When there is uncertainty in the trade-off between benefits and harms of preventive interventions,5–7 incorporation of patients’ preferences is appropriate and important.8 Accordingly, patients may decide whether to accept or reject such an intervention based on weighing the harms, cost and inconvenience of taking lifelong medication against the potential long-term benefits.9 10
Despite the growing acknowledgement of the importance of patient and public involvement in the development of CPGs, current CPGs focus primarily on the medication effectiveness and often fail to highlight uncertainty and reconcile patients’ preferences and values with the guideline recommendations.11 In addition, CPGs’ recommendations are often used as a measure of the quality of care provided by clinicians and organisations.12 13
For instance, the most recent update of the US and UK CVD risk assessment and prevention guidelines have recommended the use of statins among people previously considered at low risk of CVD, setting the threshold to commence statins at a risk of a CVD event in 10 years of 7.5%.14 15 However, this threshold reflects a value judgement about the balance of potential harms and benefits of taking statins, which some patients may not find it justifiable for taking statins.
Therefore, the purpose of this systematic review was to summarise current evidence regarding the minimum acceptable risk reduction of a cardiovascular event that patients feel would justify their taking daily preventive medication. This information is helpful both for patients to actively participate in the decision-making process,16 and guideline panels to be informed of the best evidence regarding the patients’ values and preferences in making trade-offs between desirable and undesirable consequences of such an intervention.17
Methods
A protocol for this systematic review was developed in advance (available from the authors on request).
Information sources and search methods
We developed, with the help of a medical librarian experienced in systematic reviews, a search strategy using a method of forward and backward citation analysis. We used Web of Science database to track the forward and backward citations of a set of five key articles until 15 November 2016. The index articles for our citation analysis were a relevant systematic review,18 and four other articles were identified as important in this area.9 10 19 20 Searching continued backward and forward until no further relevant studies are found. Citation analysis can evade the time-consuming and the complex nature of the standard search strategies, in areas where indexing is unlikely to retrieve relevant articles with an acceptable accuracy rate.21–23
Eligibility criteria
All published quantitative primary studies were eligible, irrespective of the study design. We included studies involving adult participants who made a decision about a cardiovascular preventive medication whether in a real-life (actual) or a hypothetical (analogous) scenario.
Studies were eligible if they assessed the minimum acceptable benefit (CVD risk reduction) of a CVD preventive medication among a sample of the general population and provided a quantitative estimate of the risk reduction (in absolute values) required by patients to make daily medication worthwhile. Absolute risk reduction estimates could be presented in the format of prolongation of life (POL), absolute risk reduction (ARR) or number needed to treat (NNT). Studies that provided a descriptive or qualitative estimate of risk reduction or a quantitative estimate of relative risk reduction (without baseline risk) were excluded.
Selection of studies
Two authors independently screened for eligibility the titles and abstracts of identified articles. We retrieved the full text of studies that potentially met the eligibility criteria. From the full texts, two authors independently assessed study eligibility. When more than one publication of the same study existed, the publication with the most complete data was included. We resolved any disagreement by discussion. Reasons for exclusion of studies were documented.
Data extraction
Two authors independently abstracted data, using a standardised data extraction form. The abstracted data included: (1) general: title, authors, country, language and year of publication, duplicate publications and sponsoring; (2) participants: sample size, baseline characteristics and study setting; and (3) scenario: hypothetical/real, type of risk presentation format (POL, ARR or NNT), method for eliciting patients’ preferences (eg, discrete choice), medication characteristics (side effects, cost and burden) and the target adverse event (mortality or morbidity).
Assessment of the methodological quality and risk of bias
Included studies were independently assessed by two authors using a modified version of the risk of bias in prevalence studies assessment tool,24 which includes the following items: representation, selection, response rate and data collection. We assessed the adequacy of each item: ‘low’, ‘unclear or ‘high’ risk of bias.
Data synthesis
For each included study, we extracted or calculated the average 5-year ARR or NNT or POL required by the participants to commence a CVD preventive medication. We reported the ranges (and sample size-weighted averages) of 5-year ARR or NNT or POL across included studies. A meta-analysis was not possible due to the heterogeneity in studies’ methods and outcomes.
Results
We screened 341 studies (after removal of duplicates), of which 238 were classed as ineligible based on titles or abstracts. Of the remaining 103 full texts, 22 studies with a total of 17 751 participants were included (figure 1).
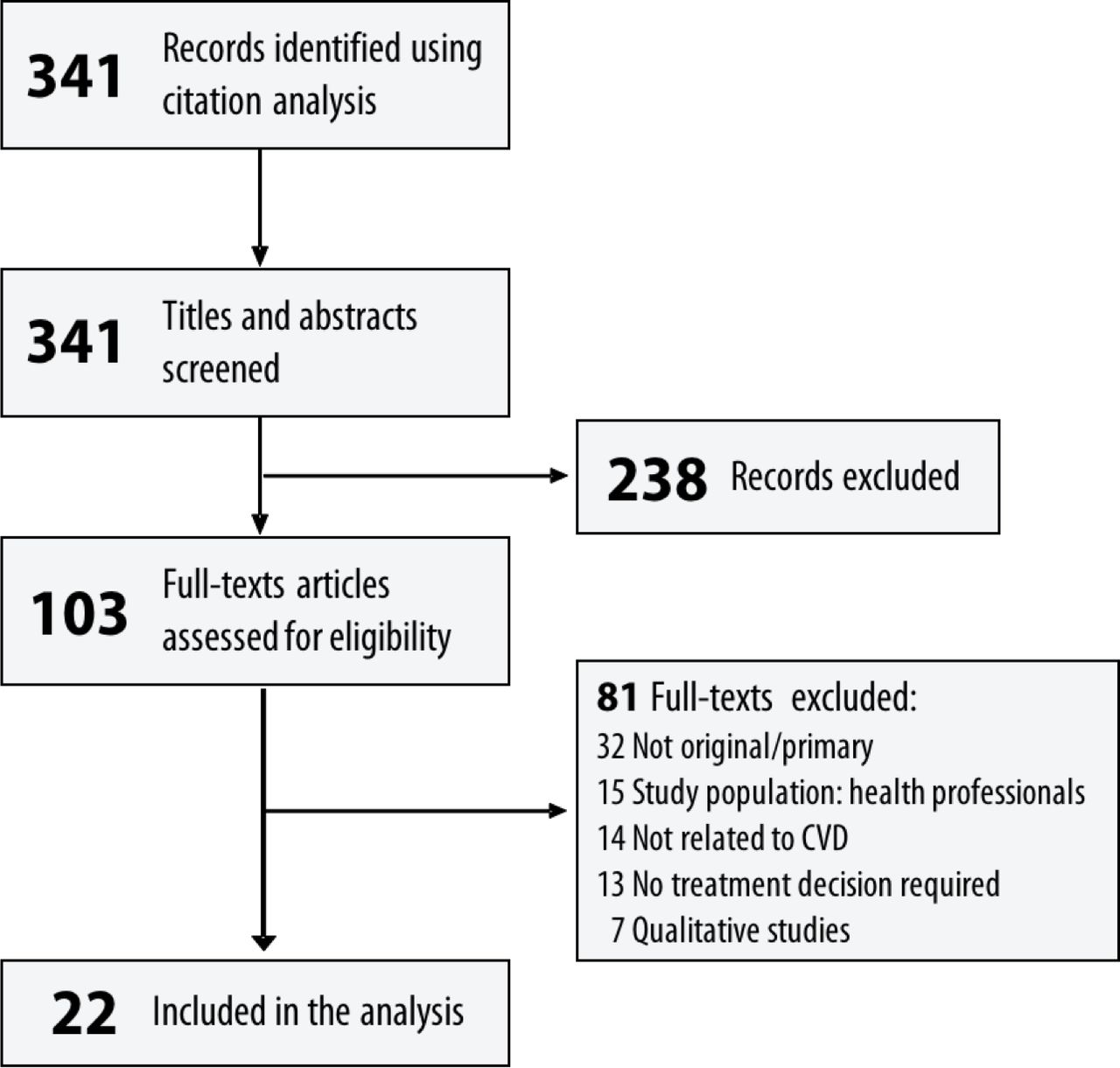
Summary of flow of information through the systematic review process (PRISMA Flow Diagram).
Study publication dates ranged from 1995 to 2014; study sample size ranged from 58 to 2978, with an average of 807 participants. Three studies were internet based (one from USA, one from Norway and one from USA and Norway), while the remaining studies were conducted in seven countries: six in UK, five in Denmark, two in Norway, two in New Zealand, two in USA and two in Canada. The 22 included studies contributed 63 estimates of minimum acceptable risk reduction: 14 studies contributed 28 estimates in the form of NNT; 12 studies contributed 22 estimates in the form of ARR and 6 studies contributed 13 estimates in the form of POL. Participants were sampled from the general population in 13 studies (59%) and from primary care settings in nine studies (41%). Most studies elicited participants’ preferences using single-choice questions (n=16; 70%). Other methods were multiple-choice questions (n=4), iterative process (n=1) or trade-off method (n=1). The most frequent method of data collection was in-person interviews (n=12; either telephone or face to face); the remaining studies used surveys to collect data from the participants (either mailed or internet-based survey). Characteristics of included studies are shown in table 1.
Characteristics of included studies
The results of the quality assessment (figure 2) showed that half of the studies truly represented the general population (n=11). Few studies (n=3) had a response rate of ≥75%, but random selection or census had been undertaken in most studies (n=17). Data had been collected using the same methods from all participants in most included studies (n=17).

Risk of bias assessment: authors’ judgements about each risk of bias item: (A) for each included study (risk of bias graph); and (B) presented as percentages across all included studies (risk of bias summary). Representation: was the sampling frame a true or close representative of the target population/general population; selection: was some form of random selection used or a census undertaken; non-response: was the likelihood of non-response bias minimal (low risk: ≥75%; high risk: <75%); data collection: were data collected directly from participants and if the same mode of data collection used for all participants.
Prolongation of life
In studies that presented the CV benefits framed as POL, 39%–73% of the participants (average 54%) would consider taking cardio-preventive medication. This decreased to 39%–54% (average 48%) when we only considered preventive medications that prolonged their life by <8 months, and increased to 56%–73% (average 64%) when the analysis was restricted to studies presented POL ≥8 (figure 3 and supplementary table 1).

Minimum acceptable risk reduction in cardiovascular events (expressed as prolongation of life) required by the patients to justify taking daily preventive medication. Bubble graph showing the percentage of participants of included studies that could accept taking a medication against the potential prolongation in life (in months in logarithmic scale) for such a medication; the bubble area represents the sample size.
Absolute risk reduction (5 years)
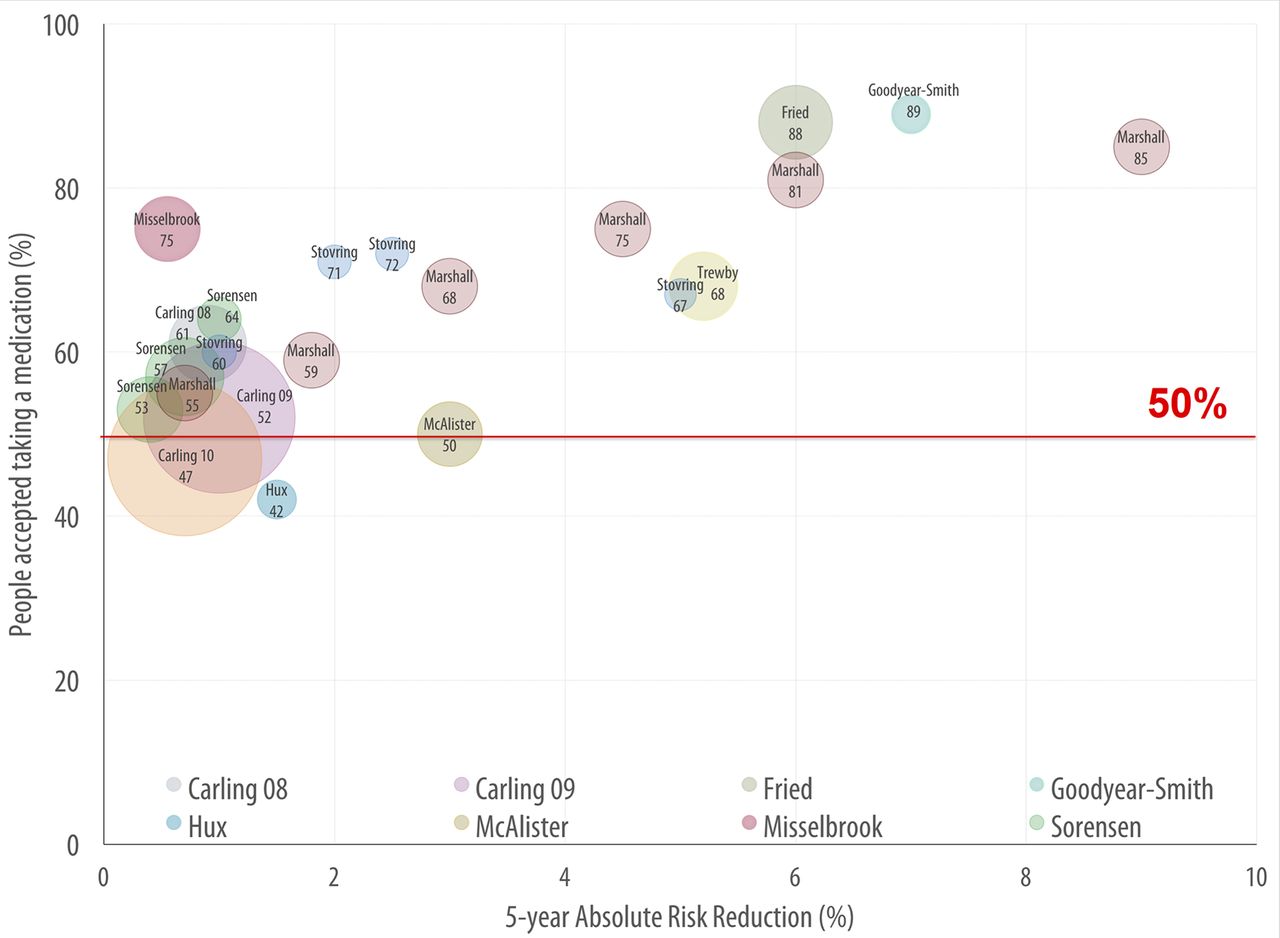
In studies that presented the CV benefits in term of ARR, 42%–89% of the participants (average 60%) would consider taking the CVD preventive medication. This decreased to 42%–72% (average 54%) when we only consider studies where medication reduced the 5-year absolute CV risk by <3%, while this percentage increased to 50%–89% (average 77%) when we consider studies presented ARR ≥3% (figure 4 and supplementary table 2).
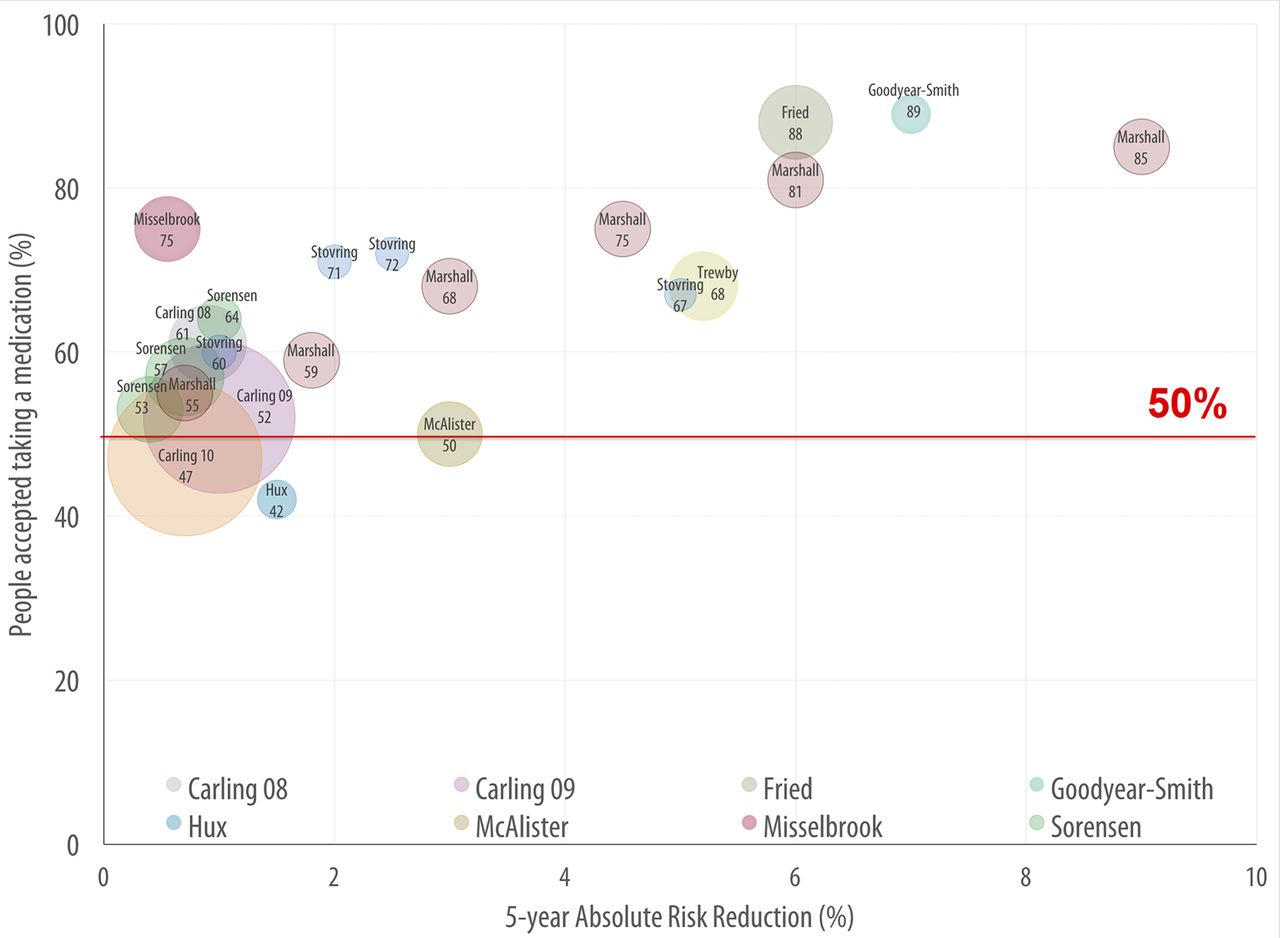
Minimum acceptable risk reduction in cardiovascular events (expressed as ARR) required by the patients to justify taking daily preventive medication. Bubble graph showing the percentage of participants of included studies that could accept taking a medication against the 5-year absolute risk reduction in cardiovascular events that can be gained by such a medication; the bubble area represents the sample size.
Number needed to treat (5 years)
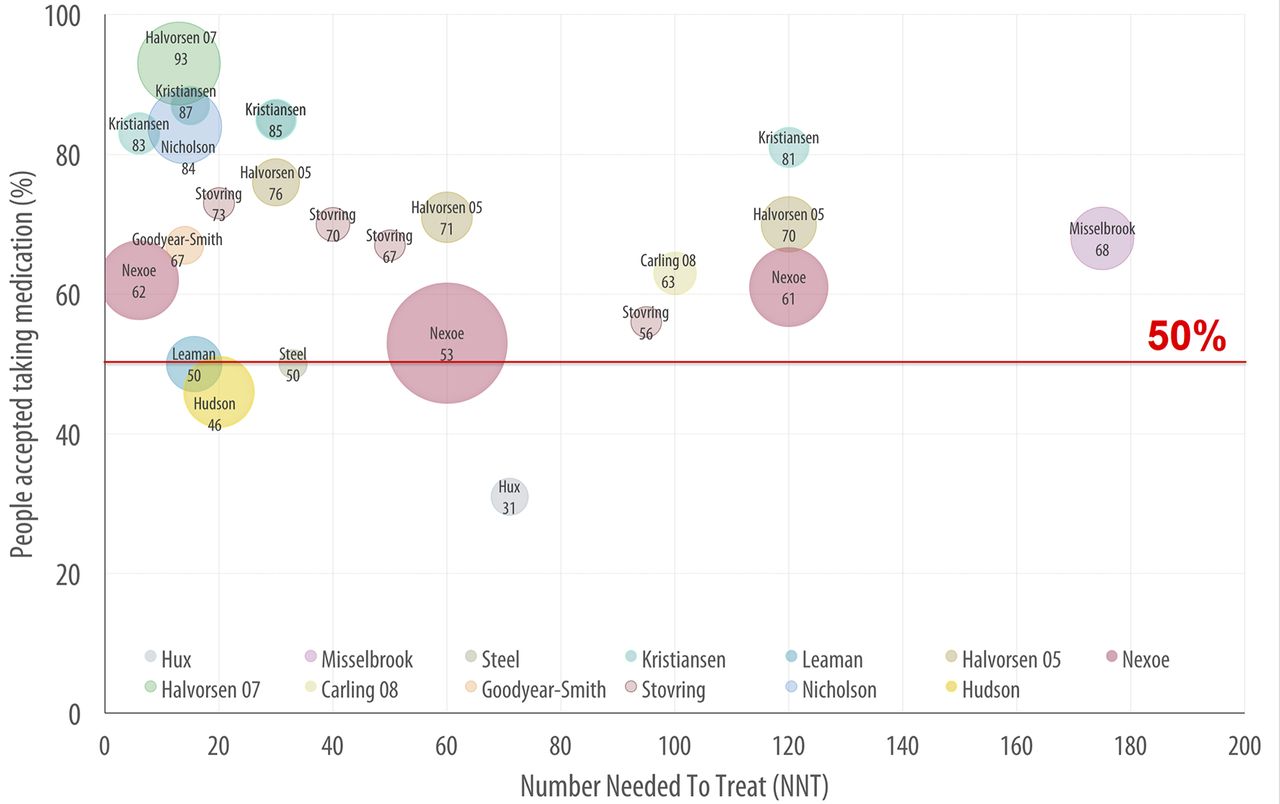
In studies that presented the CV benefits in term of NNT, 31%–87% of the participants (average 64%) would consider taking cardio-preventive medications. This decreased to 31%–81% (average 60%) when we only considered studies presented a medication needed to be taken by more than 30 persons to prevent one event while this percentage increased to 46%–87% (average 71%) when analysis restricted to studies presented NNT ≤30 (figure 5 and supplementary table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Minimum acceptable risk reduction in cardiovascular events (expressed as NNT) required by the patients to justify taking daily preventive medication. Bubble graph showing the percentage of participants of included studies that could accept taking a medication against the number of individual needed to be treated for 5 years to prevent one cardiovascular event; the bubble area represents the sample size.
Factors affecting the decision to commence a CVD preventive therapy
Some studies explored other factors that would affect the decision to take a medication. These factors help to explain some of the heterogeneity observed between studies.
Probabilistic versus deterministic ‘fixed’ presentation of risk
One study found that participants were more likely to agree to a CVD preventive therapy when the benefits were presented as a certain, short, postponement of a heart attack (182/456; 40%) compared with an equal average but uncertain ‘probabilistic’ long postponement of the outcome (153/452; 34%).19 This cognitive bias has been also shown by Finegold et al. 25 Participants presented with a certain 1 year life gain were more likely to accept a medication than when presented with a 10% chance of 10 year life gain (56% vs 45%).25 However, if participants were presented with two gains that were not probabilistically equivalent, they preferred the therapy that provides the larger gain whether presented as a certain or uncertain benefit.25
Positive versus negative framing
Carling et al 26 found that participants were more likely to agree for a CVD medication when the risk reduction was framed negatively (66%) than positively (56%) or compared with informed information that included positive and negative format together (40% and 46%, respectively). Similarly, Goodyear-Smith et al 27 found that participants were more likely to agree to taking a CVD medication when the benefits were framed negatively (89%) than positively (80%).
Risk presentation format
Stovring et al 28 found that the proportion of respondents willing to take a medication to prevent CVD was higher when the benefit was presented as either ARR (expressed in natural frequencies) or NNT compared with POL. Notably, POL was found to have the least concordance with final decisions that were based on comprehensive information (ARR, NNT, RRR and pictorial presentation). However, another study found more patients considered taking medication when the results were presented as ARR (85%) than NNT (67%).27 Carling et al 29 compared different presentations of risk reduction and found that participants were more likely to consider a medication when the benefit presented as relative risk reduction, but natural frequencies were scored the highest in preference, understanding and satisfaction with the presented information and confidence in the decision.
Adding adverse effects
Fried et al 30 asked community-living older persons their willingness to agree to CVD preventive medications with varying degree of benefits and harms (both type and severity) and found that about a half of the respondents who initially agreed to a medication with average benefit with no adverse effects were unwilling or uncertain about taking the same medication if it was associated with even mild fatigue and nausea, and only 3% of them would agree to a medication that had adverse effects that could affect their activities of daily living.
History or high risk for CVD
The presence of known risk factors or a history of CVD might also affect the decision to take the medication. For instance, Misselbrook and Armstrong31 found that patients with known high blood pressure were more likely to agree to a CVD preventive medication than participants with normal blood pressure, which has been also found by McAlister et al.32 Similar findings were also shown by Trewby et al 33 comparing participants with a history of CVD and taking medications to patients either without CVD history but taking a preventive medication or without CVD history and taking no medication. Similarly, Dahl et al found that previous history of myocardial infarction (OR: 2.5; 95% CI 1.3 to 5.0) and elevated cholesterol level (OR: 1.9; 95% CI 1.8 to 2.6) significantly increased the odds of consenting to medication.34 Fried et al found that participants who rated their health as poor/fair were more likely to consider taking a medication than those rated their health as excellent/very good.30 However, two other studies found no association between self-reported health, CVD history and the odds of considering taking medication.19 35
Participant baseline characteristics
Male gender was found to be significantly associated with considering taking a medication in Dahl et al 34 Halvorsen and Kristiansen36 and Hudson et al 3 but not in Halvorsen et al 19 Nexøe et al 37 and Kristiansen et al.35 Older age and higher education level was significantly associated with considering taking a medication in Halvorsen et al 19 and Kristiansen et al 35 but not in Nexøe et al 37 Halvorsen and Kristiansen36 and Dahl et al.34
Perspective of patients versus clinicians
McAlister et al 32 compared the minimum gain in ARR to consider taking CVD medication between hypertensive patients (with no overt CVD) and family physicians and found that patients demand greater benefits before agreeing to a CVD preventive medication compared with physicians. Similarly, Steel38 found that the gain in ARR to agree to an antihypertensive medication was lower among consultant physicians than general practitioners and highest among the general public.
Discussion
Results of the 22 studies in this systematic review suggest that an implicit assumption in cardiovascular prevention guidelines—that participants accept the amount balance between benefits and harms—may not be concord with patient preferences. Even in the studies where people were presented with an idealised tablet with no side effects, more than one-third stated they would not consider taking a medication that could prevent their 5-year absolute risk of a cardiovascular event by an ARR of 5% or more. This gain is rarely achieved by CVD medication (eg, statin reduce the relative risk of a CVD event by about 5-year CV absolute risk by about 30%.39 40 Moreover, considerable variations were observed in the patients’ preferences of the minimum acceptable risk reduction of cardio-preventive medication.
Several factors may explain the wide variation in patients’ preferences both within and across included studies, such as whether patients are already taking a preventive medication, and the way that the risk reduction has been communicated to the participants (eg, risk presentation format and framing effect). A recent systematic review of risk communication found that the various risk presentation formats might have different effects on the decision to consider taking medication.41 However, it is important to distinguish between the persuasiveness of the risk presentation formats and the clarity and understandability of the format.18 Methods used to elicit preferences (eg, single-choice options and trade-off) as well as those used to collect data (face-to-face interviews and mailed questionnaire) may also contribute to variation observed. Lastly, the characteristics of the medication presented to participants may also have affected their decisions. An ideal medication (free of charge and no side effects) is more likely to be accepted compared with a real-life medication with costs and potential side effects.
Thus, when patients’ preferences vary widely, preventive guidelines should be wary of setting a single risk threshold for the initiation of a preventive treatment based on the effectiveness of the medication. Any threshold point or range should be based on the balance of benefits and downsides, which should be informed by patients’ value and preferences.
Strength and limitation
The heterogeneity of methods used to assess the preferences, including trade-off method, iterative process and single-choice questions, is both a strength and limitation of our study. The inclusion criteria meant that a wide variety of estimates could be included in the review, but owing to this heterogeneity of the methods and outcomes, we could not calculate quantitative summary estimates of the minimum acceptable risk reduction, which is common in systematic reviews in this field.17 42 43 Moreover, most of the included studies have not been designed primarily to assess our research question but to examine other issues such as response to framing. In addition, the review only considers those factors reported in the included studies. Another potential limitation is the risk of missing relevant articles because of the use of citation analysis as a search strategy. However, studies in other areas suggest that the accuracy rate of this method is acceptable (eg, using citation analysis, Janssens and Gwinn retrieved about 94% (75–100%)%) of all included articles retrieved using traditional method in 10 meta-analyses).23 Thus, we think that our overall results and conclusion are unlikely to be affected.
Implication for clinical practice
Patients’ preferences should be considered in both guideline development and clinical care. Patients’ representatives and member of the public should be actively involved in guideline development panels.44 Future guidelines must consider more than the evidence of medication effectiveness in establishing treatment thresholds: systematic reviews of patients’ values and preferences should also be conducted to inform guideline recommendations. Given the heterogeneity in individual preferences, guidelines should include strategies to help clinicians incorporate patients’ preferences and values to make informed decisions. This can be achieved by promoting choice, providing adequate information about the benefit and risks of medication, and the level of uncertainty in the evidence, and highlighting that guideline recommendations support, but do not substitute for, clinical judgement and individualised decision making. Visual aids (eg, icon arrays or risk pictograph) to communicate risk reduction might be used since evidence shows that such aids improve patients’ understanding and satisfaction.41 This also implies that the ‘do or do not’ style of recommendations should generally be discouraged and that preference-sensitive recommendations should not be used as indicators of quality of care (quality measures).
Clinicians often fail to accurately identify patient preferences—a problem termed silent misdiagnosis,45 and hence guidelines should include tools that promote shared decision making where intervention choices can be tailored to patients’ clinical characteristics and to their values and preferences. This means that guideline recommendations should be used as a starting point for the individual patient–clinician decision-making process. In addition, patient versions of guidelines, as well as decision aids tools, should be developed and disseminated along with the guidelines.
Implication for future research
This systematic review highlights the need for standardising the key measures of patient preferences that might be used to inform guidelines. Future research could gain from using well-established methods for preference elicitation used in other disciplines (eg, health economics) to develop a valid, reliable and sensitive measure of patient preferences in a medical decision-making context. Moreover, a systematic review of qualitative studies regarding the factors affects the individual decision of CV preventive medication is also warranted.
Conclusion
Even for a side effect-free, costless medication, many patients require a substantial risk reduction to consider taking a preventive medication. However, the range of answers is very wide with some accepting any gain and other not willing to consider medication with any gain. Guidelines and clinical consultations need to account for both these average and individual values in setting risk thresholds.
Acknowledgments
We would like to thank Ms Sarah Thorning for her help with the literature search.
References
Footnotes
Twitter Follow Loai Albarqouni at @lnb6des, and Jenny Doust at @jadoust, and Paul Glasziou at @paulglasziou.
Contributors LA, JD and PG designed the study. LA, JD and PG screened the articles. LA, JD and PG extracted data. LA drafted the original manuscript, and all authors revised the paper. LA is the guarantor of the study.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: Dr Glasziou reports grants from National Heart Foundation prior to the conduct of this study. No support from any organisation for the submitted work; no other relationships or activities that could appear to have influenced the submitted work.
Patient consent This study is a systematic review, hence, no direct involvement of human subjects.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data extracted from the included studies are available on request from the corresponding author.