Article Text

Statistics from Altmetric.com
The application of high-quality evidence to clinical decision making requires that we know how to access that evidence. In years past, this meant literature searching know-how and application of critical appraisal skills to separate lower from higher quality clinical studies. However, over the past decade, many practical resources have been created to facilitate ready access to high-quality research. We call these resources “pre-appraised” because they have undergone a filtering process to include only those studies that are of higher quality and they are regularly updated so that the evidence we access through these resources is current.
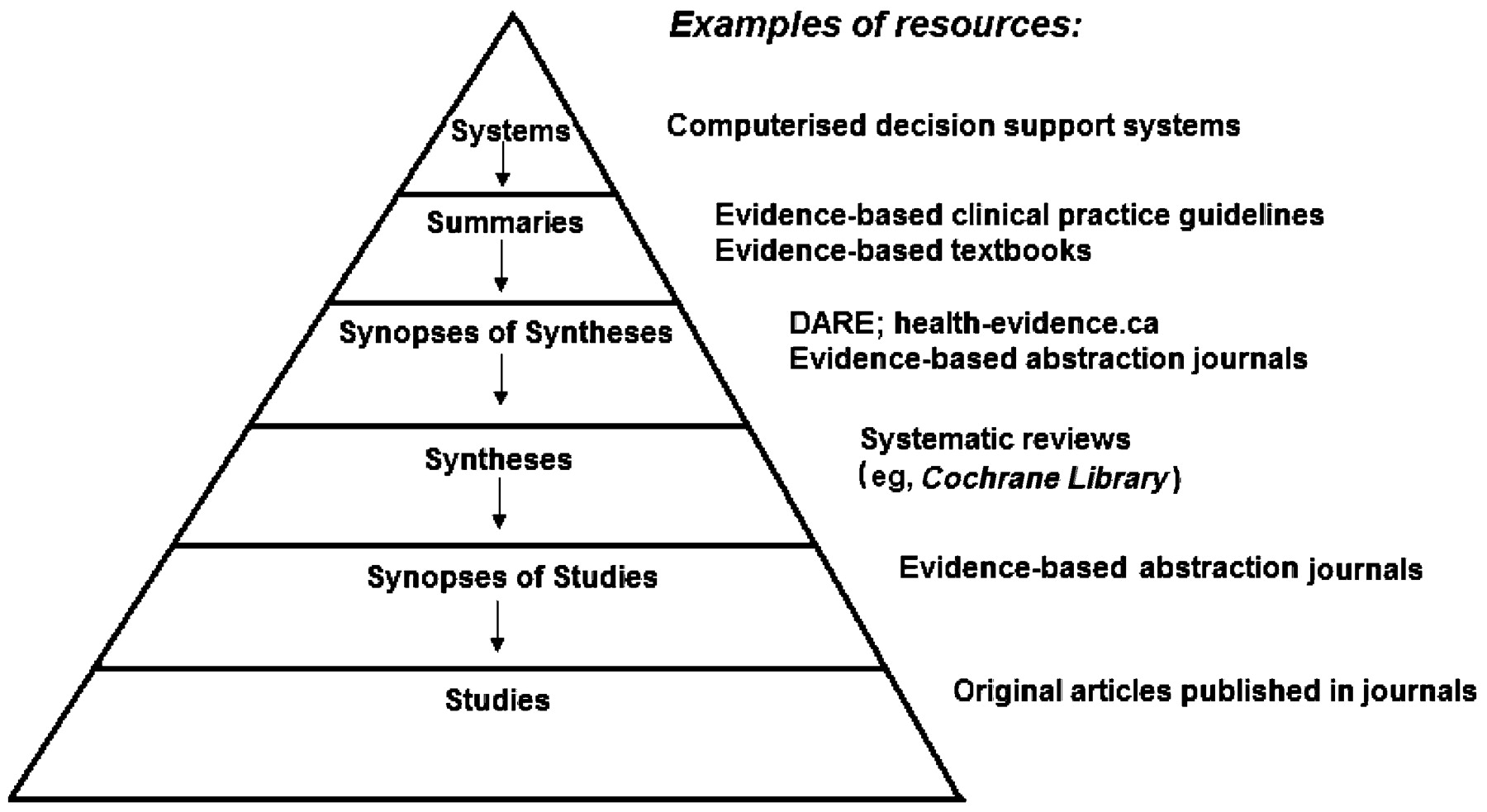
To facilitate use of the many pre-appraised resources, Haynes proposed a “4S” model,1 which he then refined into a “5S” model.2 The 5S model begins with original single studies at the foundation, and building up from these are syntheses (systematic reviews such as Cochrane reviews), synopses (succinct descriptions of selected individual studies or systematic reviews, such as those found in the evidence-based journals), summaries, which integrate best available evidence from the lower layers to develop practice guidelines based on a full range of evidence (eg, Clinical Evidence, National Guidelines Clearinghouse), and at the peak of the model, systems, in which the individual patient’s characteristics are automatically linked to the current best evidence that matches the patient’s specific circumstances and the clinician is provided with key aspects of management (e.g., computerised decision support systems).2
When we described the 5S model to colleagues at home and abroad, some queried whether a synopsis of a single study and a synopsis of a systematic review are equivalent as indicated by their single appearance in the model. In the hierarchy of evidence, a systematic review bests a single study, so we are adding a layer to the model to distinguish the 2 types of synopses.
The 6S model
In the 6S model (Figure), we now have synopses of studies in the second layer from the bottom and synopses of syntheses in the fourth layer from the bottom, which more accurately depicts their rigour.

{kind=link}
The 6S hierarchy of pre-appraised evidence
When using this model to guide clinical decision making, begin your search at the highest possible layer in the 6S model. In an ideal situation, this would be the systems layer. An evidence-based clinical information system integrates and concisely summarises all relevant and important research evidence about a clinical problem, is updated as new research evidence becomes available, and automatically links (through an electronic medical record) a specific patient’s circumstances to the relevant information.1 In these computerised decision support systems (CDSSs), detailed individual patient data are entered into a computer program and matched to programs or algorithms in a computerised knowledge base, resulting in the generation of patient-specific assessments or recommendations for clinicians.3 For example, CDSSs exist to manage oral anticoagulation in nurse-led primary care clinics in the UK4 ,5 and to increase inpatient influenza vaccination.6 Although electronic medical systems that incorporate computerised decision support rules have been shown in randomised trials to improve the process, and sometimes the outcome,3 of care, few such systems are currently available. If your electronic medical record system incorporates a CDSS that reliably links a patient’s characteristics with current evidence-based guidelines for care, you need not go further down the model.
If a CDSS does not exist, the next best step is to look for summaries. These include clinical pathways or textbook summaries that integrate evidence-based information about specific clinical problems and provide regular updating. Clinical Evidence (www.clinicalevidence.com), Dynamed (www.ebscohost.com/dynamed/default.php), and the Physicians’ Information and Education Resource (PIER) (pier.acponline.org) use explicit review processes to find and appraise evidence about the management of a wide range of clinical problems. UpToDate (www.uptodate.com) also provides evidence-based information about specific clinical problems and is regularly updated, but the review process is not explicit.
Evidence-based, current clinical practice guidelines (CPGs), which are “systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances,”7 are also examples of “summary” level evidence. A CPG should be based on comprehensive searches and appraisal of the literature (ideally current systematic reviews, if they exist), and each recommendation should be accompanied by levels of evidence. Users should consider acting only on those recommendations based on high-quality evidence. High-quality CPGs are produced by numerous organisations, such as the Registered Nurses’ Association of Ontario (www.rnao.org) (e.g., promoting asthma control in children8) and the Canadian Diabetes Association (e.g., prevention and management of diabetes9). While the National Guidelines Clearinghouse (www.guideline.gov) is a freely accessible comprehensive source of CPGs, readers should keep in mind that not all CPGs are created equal—be sure that the CPG is current and that the recommendations are evidence-based (i.e., accompanied by levels of evidence).
When a summary does not exist for a clinical problem, then synopses of syntheses are the next best source. A synthesis or systematic review is a comprehensive summary of all the research evidence related to a focused clinical question. It involves a multi-step process in which the question is formulated, the relevant studies are identified and appraised for study quality, relevant study findings are extracted and synthesised either quantitatively (in the form of meta-analysis) or non-quantitatively, and conclusions are drawn. Given that many busy clinicians do not have the time to review detailed systematic reviews, a synopsis that summarises the findings of a high-quality systematic review can often provide sufficient information to support clinical action. These synopses can be found in the evidence-based abstraction journals such as ACP Journal Club (www.acpjc.org), Evidence-Based Medicine (ebm.bmj.com), Evidence-Based Mental Health (ebmh.bmj.com), and Evidence-Based Nursing (ebn.bmj.com). They can also be found in the Database of Abstracts of Reviews of Effects (DARE) (www.crd.york.ac.uk/crdweb/Home.aspx?DB = DARE), which contains summaries of syntheses that have met strict quality criteria and critical commentaries on the quality of the syntheses. The advantages of finding a relevant synopsis of a synthesis are 2-fold: first, the synopsis provides a convenient summary of the corresponding synthesis, and second, it is often accompanied by a commentary that addresses the methodological quality of the synthesis and the clinical applicability of its findings. A limitation is that it takes time to prepare a systematic review after the publication of original studies, and a synopsis extends this timeline even further.
If more detail is needed or no synopsis exists, then databases of syntheses (systematic reviews) are available, notably ACPJC PLUS (plus.mcmaster.ca/acpjc), EvidenceUpdates (http://plus.mcmaster.ca/evidenceupdates), and Nursing+ (plus.mcmaster.ca/np), which contain systematic reviews from >160 journals and the Cochrane Library. The Cochrane Library (www.thecochranelibrary.com/) houses syntheses about the effectiveness of healthcare interventions and some diagnostic tests, and also includes the DARE database of systematic reviews. A more recent initiative, the Campbell Library (www.campbellcollaboration.org/library.php) includes syntheses related to education, criminal justice, and social welfare.
If there are no systems, summaries, synopses of syntheses, or syntheses related to the clinical problem, the next stop is synopses of single studies. As with the synopses of syntheses, the synopsis of a single study provides a brief, but often sufficiently detailed, summary of a high-quality study that can inform clinical practice. These synopses are also found in the evidence-based abstraction journals and are accompanied by commentaries that address the clinical applicability of the study findings. The advantages of a synopsis of a single study over a single study are 3-fold: first, the assurance that the study is of sufficiently high quality and clinical relevance to merit abstraction; second, the brevity of the summary; and third, the added value of the commentary.
The final stop for pre-appraised evidence, if there are no synopses of single studies, is the single original study. Studies that have met critical appraisal criteria appear in ACPJC PLUS, EvidenceUpdates, and Nursing+.
If you can’t find what you are looking for in these pre-appraised services, there are traditional non-appraised evidence services. The exemplar for these services is PubMed (www.pubmed.gov). In addition to providing access to Medline, PubMed also offers user-friendly approaches to evidence-based searching: Clinical Queries (www.ncbi.nlm.nih.gov/corehtml/query/static/clinical.shtml) for clinical research and Special Queries (www.nlm.nih.gov/bsd/special_queries.html) for health services and qualitative research, which include research methodology filters that enable searchers to quickly locate relevant and methodologically sound studies.10 Ovid Medline, EMBASE/Excerpta Medica, PsycINFO, and Ebsco CINAHL also incorporate these filters as part of their search limit features.
Searching multiple sources at once
“Federated” search engines exist for use by those who don’t know which database is best suited to answer a clinical question; examples of federated search engines include SUMSearch (sumsearch.uthscsa.edu) and TRIP (Turning Research into Practice) (www.tripdatabase.com). These search engines sort evidence across a range of databases (e.g., National Guidelines Clearinghouse, Cochrane Library, abstraction journals); however, the quality of the retrieval depends on the source, and many sources do not provide critical appraisal of evidence.
Using evidence from pre-appraised resources
Processing single studies into synopses, syntheses, and summaries takes time, and therefore, the current best evidence may not always be available in a pre-appraised resource as quickly as we would like. Indeed, there is no guarantee that high-quality evidence exists for the clinical problem of interest or that the patients studied are sufficiently similar to the patients to whom we hope to apply the results. Thus, users always must retain responsibility for use of evidence in a given clinical decision. The orderly use of current evidence-based resources, however, will often make the burden of this decision much lighter.
We are grateful to our colleagues whose feedback has encouraged us to further refine this model. We encourage readers to use this model, beginning at the top, when addressing clinically important questions. The use of these pre-appraised resources will increase the chances of efficiently finding high-quality, current evidence that is relevant to practice.
Footnotes
-
Disclaimer: Alba DiCenso is a former editor of Evidence-Based Nursing. Brian Haynes is editor of ACP Journal Club, co-editor of Evidence-Based Medicine, coordinating editor for Evidence-Based Nursing, developer of ACPJC PLUS, EvidenceUpdates, Nursing+, PubMed Clinical Queries, and PubMed Special Queries, and an evidence supplier for Clinical Evidence and PIER.