Article Text

Statistics from Altmetric.com
Practising evidence-based healthcare (EBHC) is integrating the best research evidence with clinical expertise and patients' circumstances and values.1 However, the best research evidence may seem unattainable when information is constantly developing. Finding it is daunting with numerous textbooks and guidelines, millions of studies in PubMed and many other sources. Fortunately, resources to overcome such information overload and provide rapid access to valid clinical knowledge continue to evolve.
Haynes proposed a 4S pyramid model in 2001 for practical guidance in selecting resources for rapidly finding the best evidence for EBHC.2 The 4S hierarchy has original studies already appraised for scientific merit as the foundation (‘preappraised evidence’), then progressively more clinically usable information including syntheses (systematic reviews) of evidence, synopses (structured abstracts) of preappraised studies and syntheses (systematic reviews), and at the top the most clinical workflow-specific evidence-based information systems, for example, computerised decision support systems integrated with electronic health records.
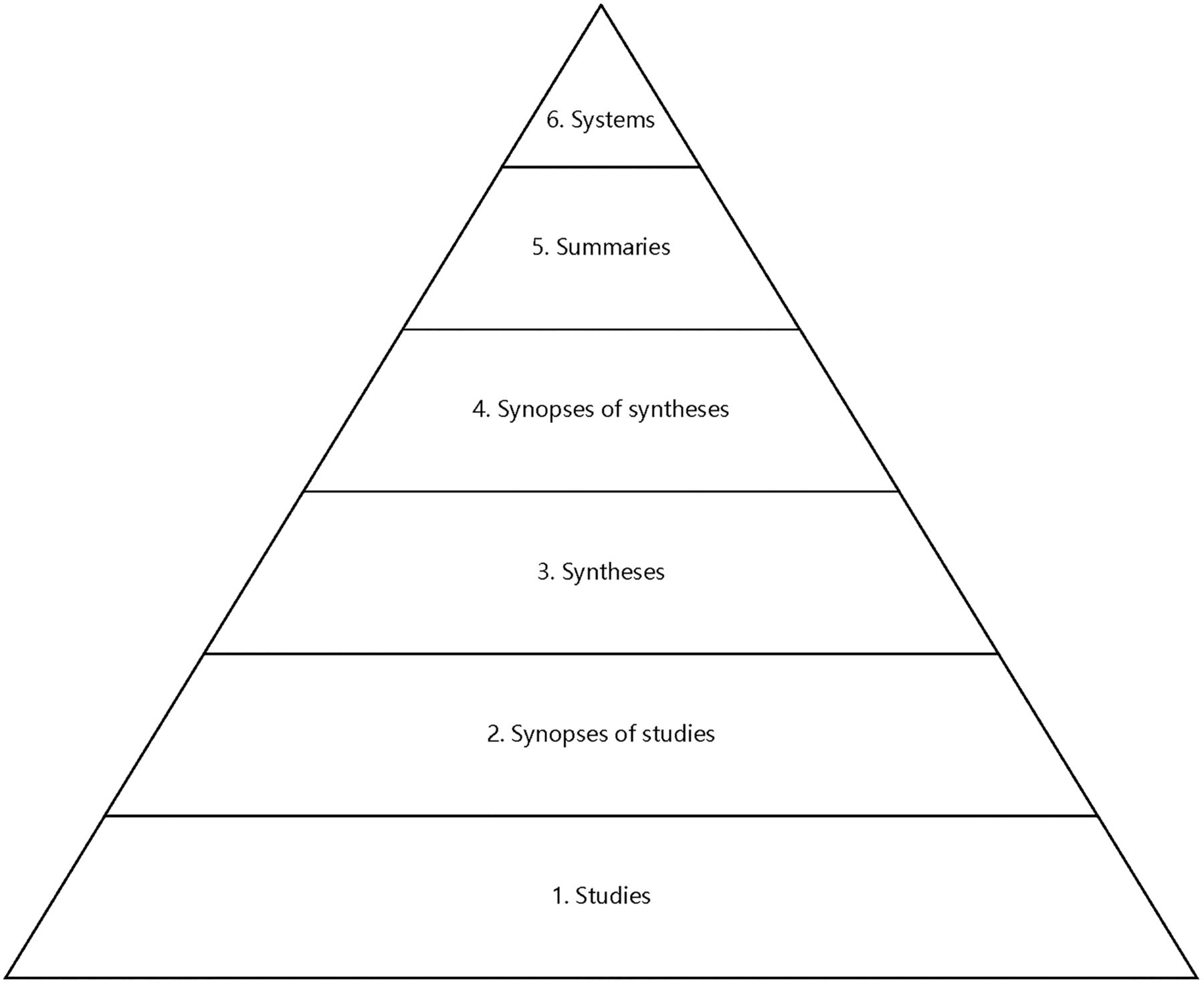
This was extended to a 5S pyramid model in 2006 by adding summaries—continuously updated, online medical texts that integrate lower levels (studies, syntheses and synopses) with clinical expertise—near the top of the pyramid, recognising that summaries could provide the fastest route to the best research evidence for preventing or managing health problems.3 The 6S model in 2009 separated synopses into synopses of studies and synopses of syntheses (figure 1).4

6S pyramid for finding preappraised evidence.4
Evidence-based information services and resources have continued to progress. Alper proposed a 9S pyramid model in 2014 to clarify how evidence-based guidelines fit in the progression from evidence to point-of-care guidance.5 Guidelines, when carried out well and current, are a collection of systematically derived recommendations integrating the best research evidence with clinical expertise and patient values.
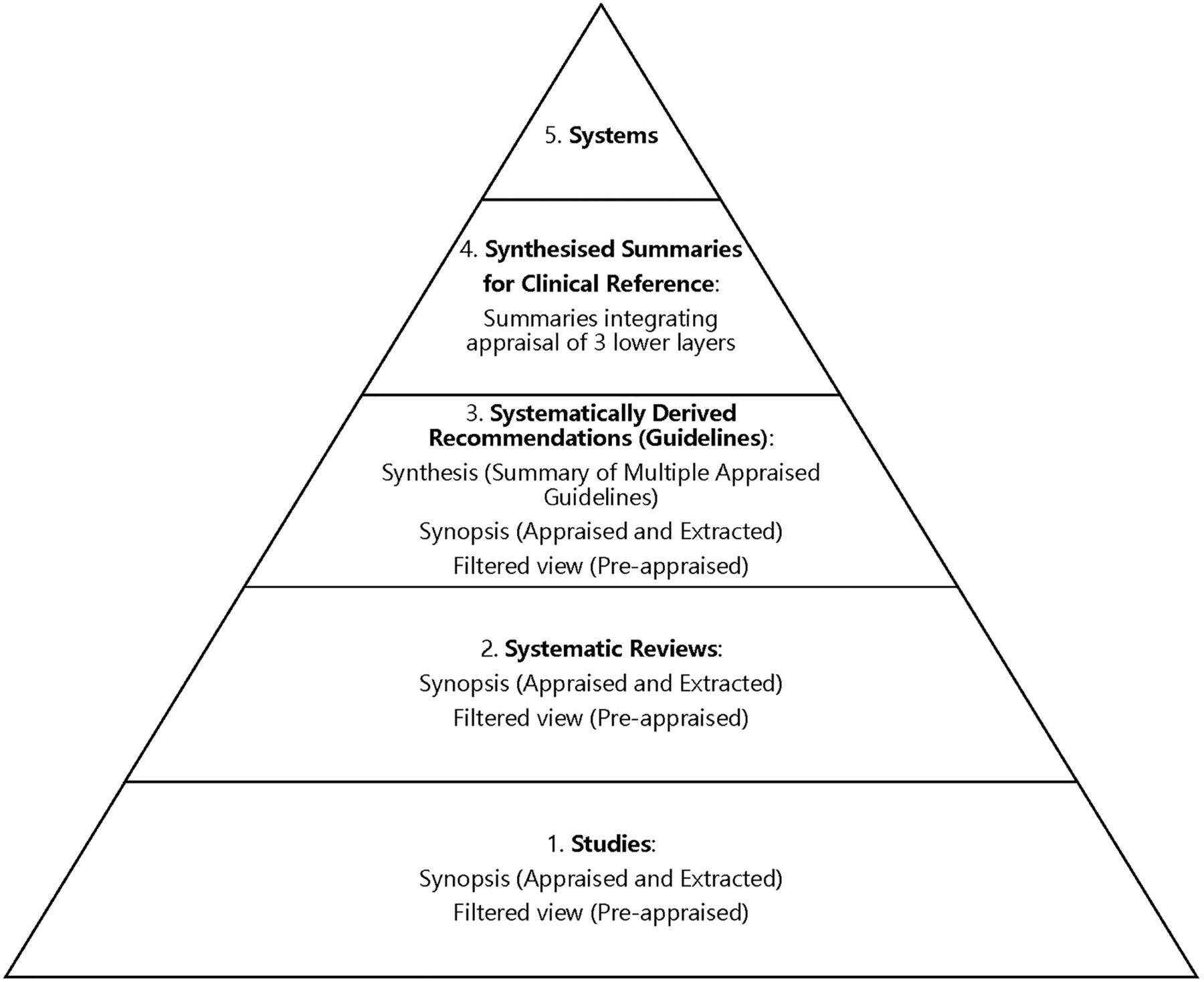
Grappling with increasing alliterations supplanting definitions (eg, syntheses are not necessarily systematic reviews), potentially increasing layers (eg, synopses of syntheses of systematically derived recommendations) and complexity overtaking usefulness of such models, we developed a streamlined fifth iteration as the EBHC pyramid 5.0 (figure 2).

{kind=link}
{kind=link}
Evidence-based healthcare pyramid 5.0 for finding preappraised evidence and guidance.
There are five levels—studies, systematic reviews, systematically derived recommendations (guidelines), synthesised summaries for clinical reference and systems. Each of these levels should build systematically from lower levels and provide substantially more useful information for guiding clinical decision-making. Within the bottom three levels, critically appraised content includes filtered (preappraised) collections of original reports, synopses of original reports (appraisal and extraction of key content), and syntheses combining multiple original reports and/or synopses. Synthesised summaries for clinical reference are resources that include all three lower layers and integrate the content meeting clinical reference needs.
When available and current, resources higher up the pyramid should be more efficient for clinicians, but two problems need to be addressed. First, it is not known in advance for any given information need whether the best results will be found at any particular level of the pyramid. One solution to this challenge is a federated search, an information retrieval technology that allows the simultaneous search of resources at multiple levels. Examples of federated searches that include evidence-based sources and layering of results consistent with this pyramid model include ACCESSSS Federated Search, MacPLUS Federated Search and TRIP Database.
Second, any result found higher up the pyramid is prone to become outdated, incomplete or even misleading as substantive changes occur in the evidence base or other levels of the pyramid that are missed or delayed in being incorporated into the higher levels, a process that often takes years.6 A solution to this challenge is a synthesis of summaries across pyramid levels with an infrastructure and commitment to rapidly integrate new evidence and guidance changes. Synthesised summaries for clinical reference provide frequently updated summaries of evidence and systematically derived recommendations and become the top level when searching for practical guidance for EBHC. Current resources providing synthesised summaries for clinical reference with varying degrees of quality, currency and comprehensiveness7–10 include BMJ Best Practice, DynaMed Plus, EBM Guidelines, Essential Evidence Plus and UpToDate.
The top of the pyramid (systems) continues to represent the scenario in which the evidence and guidance lower in the system are integrated within computerised decision support systems and electronic health records so that the features of individual patients are automatically linked with the information best suited to their care, rendering unnecessary ‘the search’ as a practitioner action. This ideal continues to be a challenge to implement in a reliable and extensive way, but Evidence-Based Medicine electronic Decision Support (EBMeDS) is now implemented at sites in several European countries.
We offer the EBHC Pyramid 5.0 as a functional model for selecting evidence-based information for clinical care and organising search retrieval for the most efficient approach to evidence-based practice. We look forward to a future where the most relevant, comprehensive, concise, context-specific synthesised evidence and guidance is immediately available in the clinical workflow, and this future is getting closer.
Footnotes
Twitter Follow Brian Alper at @BrianAlperMD
Competing interests BSA is the founding editor of DynaMed and an employee of its publisher, EBSCO and seeks collaboration with multiple entities which produce products named in this report. RBH is the founding editor of ACP Journal Club and an employee of McMaster University, which provides evidence services for a number of clinical knowledge resources including ACP Journal Club, ACP JournalWise, BMJ Best Practice, DynaMed, EBMeDS, EvidenceUpdates, ACCESSSS and MacPLUS Federated Search.
Provenance and peer review Not commissioned; internally peer reviewed.