Article Text

Statistics from Altmetric.com
Introduction
Healthcare professionals (HCP) must apply their knowledge to their practice. Consequently, the implementation of research evidence largely depends on HCPs’ knowledge, acceptance of new evidence and choices. Improving patients’ lives and the quality of healthcare requires a strong emphasis on learning by HCP, teams and patients. Mastery of any area is never the result of a single inquiry, but is instead a continuum of inquiries, searches and reflections. Spiral learning is a teaching method in which the learner progressively gains knowledge on a subject with each encounter. Usually, complexity increases with each encounter and previous material is reinforced. Spiral learning, which is currently used in medical curricula, was initially justified because learners gained expertise as they revisited topics during practical applications. Therefore, spiral learning is suggested in this paper as an appropriate process to facilitate inquiry and effective learning.
Healthcare frameworks, such as the Deming Plan-Do-Study-Act problem-solving method (PDSA), evidence-based medicine (EBM) with its five steps and the five steps of patient self-management (SM), have been applied to healthcare to help learners implement best practices in healthcare delivery. Most of these frameworks are presented as a single inquiry. This paper suggests that these frameworks will be more effective than they are at present if they follow a spiral learning approach. The continuum in spiral learning is a factor among many that determines the success of these frameworks. Others include comprehensiveness of an inquiry, learner competencies and learning context. An additional determinant is the reflection on the elements of decision-making in healthcare, such as patient values, risks versus benefits, costs and evidential strength.
Managing harms is important to safely care for patients. Every healthcare decision has a potential for harm, which could be active (eg, direct assault), come from errors in implementing care, neglecting recommended care or not preventing harm. Harm should be proactively managed or prevented via a similar spiral learning process. Finally, an important determinant is proactively targeting the learning environment to promote best evidence-based practices.
The spiral learning approach in frameworks for research-based practice
According to Donabedian, ‘quality’ is the science and technology of healthcare and the practical application of that science and technology.1 Learning to provide quality healthcare entails a series of cognitive processes that facilitate uptake of the science and its implementation, which integrates with learners’ existing skills and knowledge, both of which strengthen with time and experience. A continuum approach, spiral learning, will help learners’ to apply and integrate the best scientific and research evidence.2–6
We can apply the spiral learning approach in frameworks used in improving healthcare, professional learning and patient empowerment. Some examples are the Deming PDSA cycle,3 evidence-based medicine and the five steps in applying it4 5 and the five steps in patients’ empowerment in self-management.6
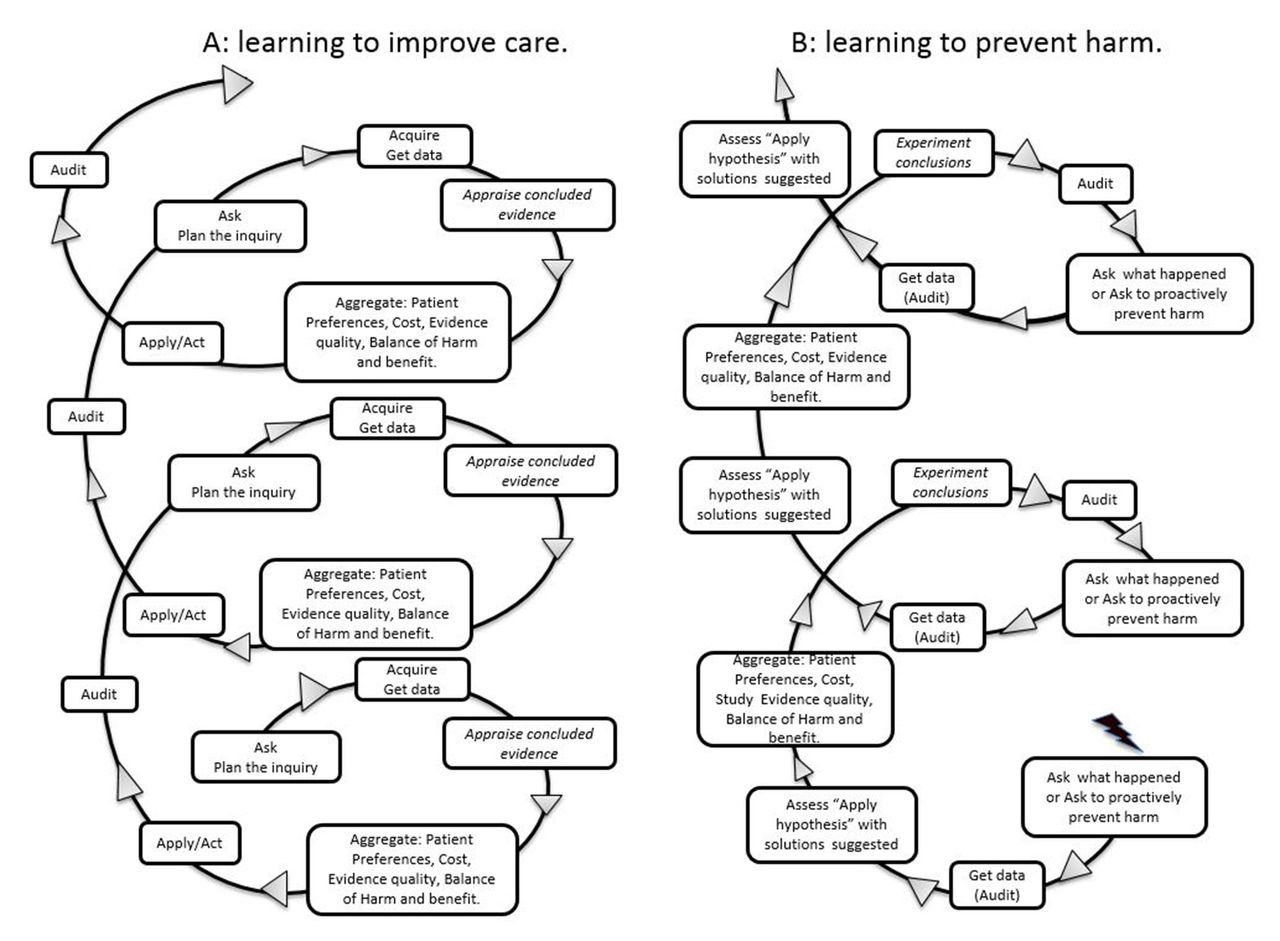
Spiral learning supports decision-making at the team, HCP and patient levels. Learning always begins with a question about a practice, disease or patient care, which triggers data collection to search for evidence. Those data are assessed and aggregated to draw conclusions for implementation. Four aspects of the evidence are considered: its strength, cost, patient values and harms versus benefits. Ultimately, the results of an implementation should trigger further inquiry. Therefore, applying evidence to practice is like a spiral of learning and practice as opposed to a stepwise process, such as EBM key steps, or a cross-sectional approach, such as PDSA. This paper proposes spiral learning, which is a shared learning process, instead of PDSA, EBM and SM, all of which influence the quality of patient care through team, HCP or patient experiences. Figure 1 illustrates the spiral approach in repeated Ask, Search, Appraise or Assess, Aggregate, Agree, Act, Audit and re-Ask cycles as a continuous accumulative process.
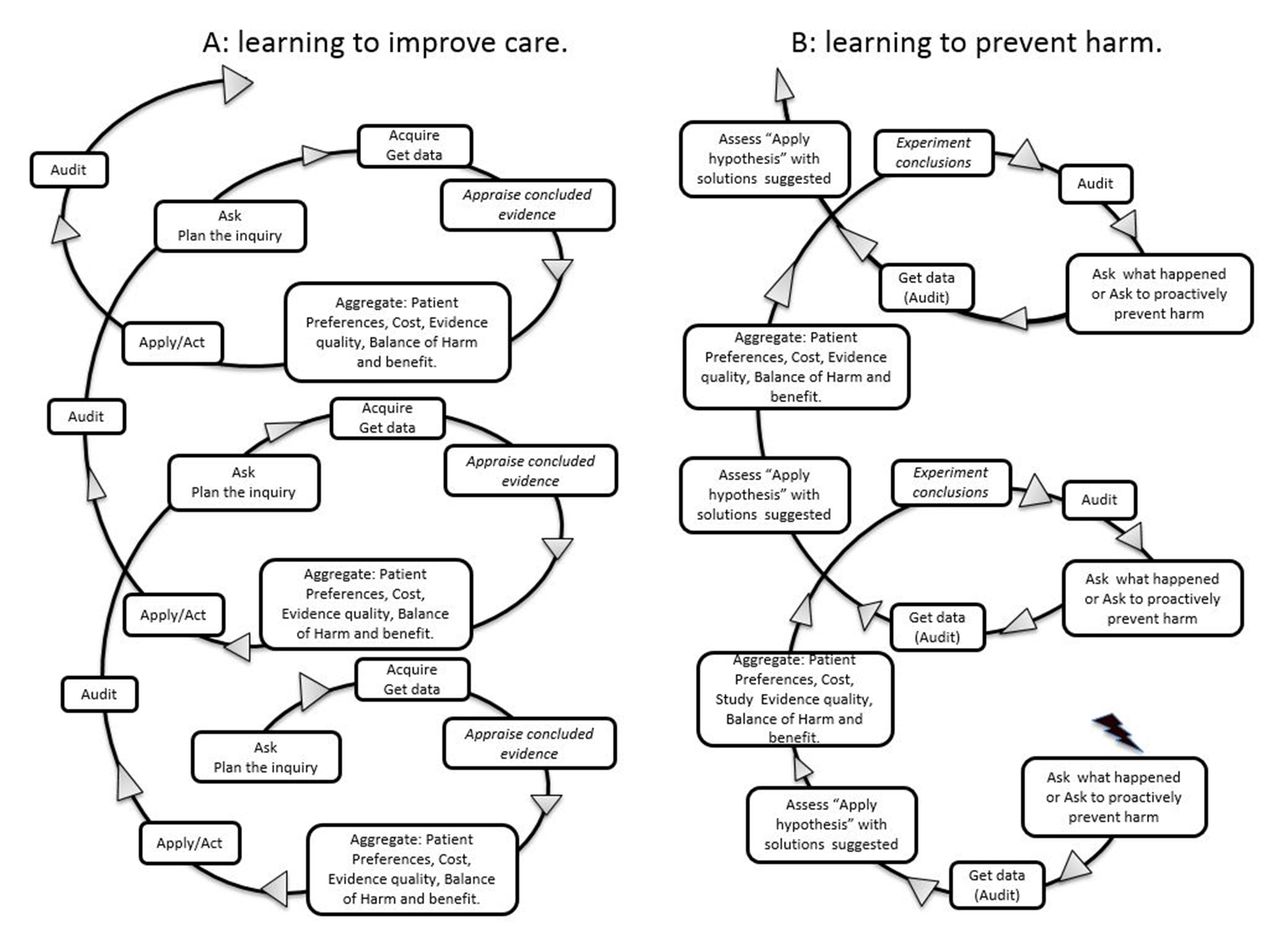
Spiral learning approach: (A) improving care and (B) prevention of harm.
Determinants of success
Comprehensive inquiry at each step
This determinant concerns previous experience and the depth of the literature review. Learners with different experiences approach questions from different perspectives, and differences in skill level accordingly influence learning, which produces a spectrum of learning outcomes from novice to expert.
Create a continuum of learning
Learning continuously progresses and triggers more learning in an upward spiral in which questions arise at progressively higher levels. Spiral learning emphasises a continuum built on previous knowledge gained because EBM knowledge is not static and frequent reconsideration is needed. As learners revisit topics in practice, they gain expertise and their questions become deeper and more complex.7 Thus, previous advocates for empowering HCP to practice EBM were correct.
Learner competencies
Learners integrate knowledge, communication skills, professionalism, ethics and practical skills in decision-making. They build skills and knowledge by deeply questioning as their expertise increases. Competent HCP can be identified by assessing their work products as an expression of their extent of knowledge and the attention given to implementing the best possible healthcare. Regardless of the extent of their knowledge and skills, a HCP’s commitment to learning and determination to implement best evidence is essential.
Learning context
Questions might be the same at different points in the learning process, whereas search methods, data and, thus, conclusions might differ. An example is the use of interventions for waiting times: if a question were about business aspects, answers from managers and clinicians would likely differ.
Fundamental reflection on the four essential elements of a conclusion (patient values, risks vs benefits, costs and strength of the evidence)
These elements are clear in the aggregate steps of the EBM and SM, but not the PDSA, approaches. This reflection leads learners towards effective decisions on knowledge application and avoids blind implementations of research findings. Evidence is implemented in practice after decisions are made, which is followed by audits of outcomes. Then, the learner returns to the spiral, but at a higher level, with deeper questions based on previous knowledge, and the spiralling continues.
Special applications
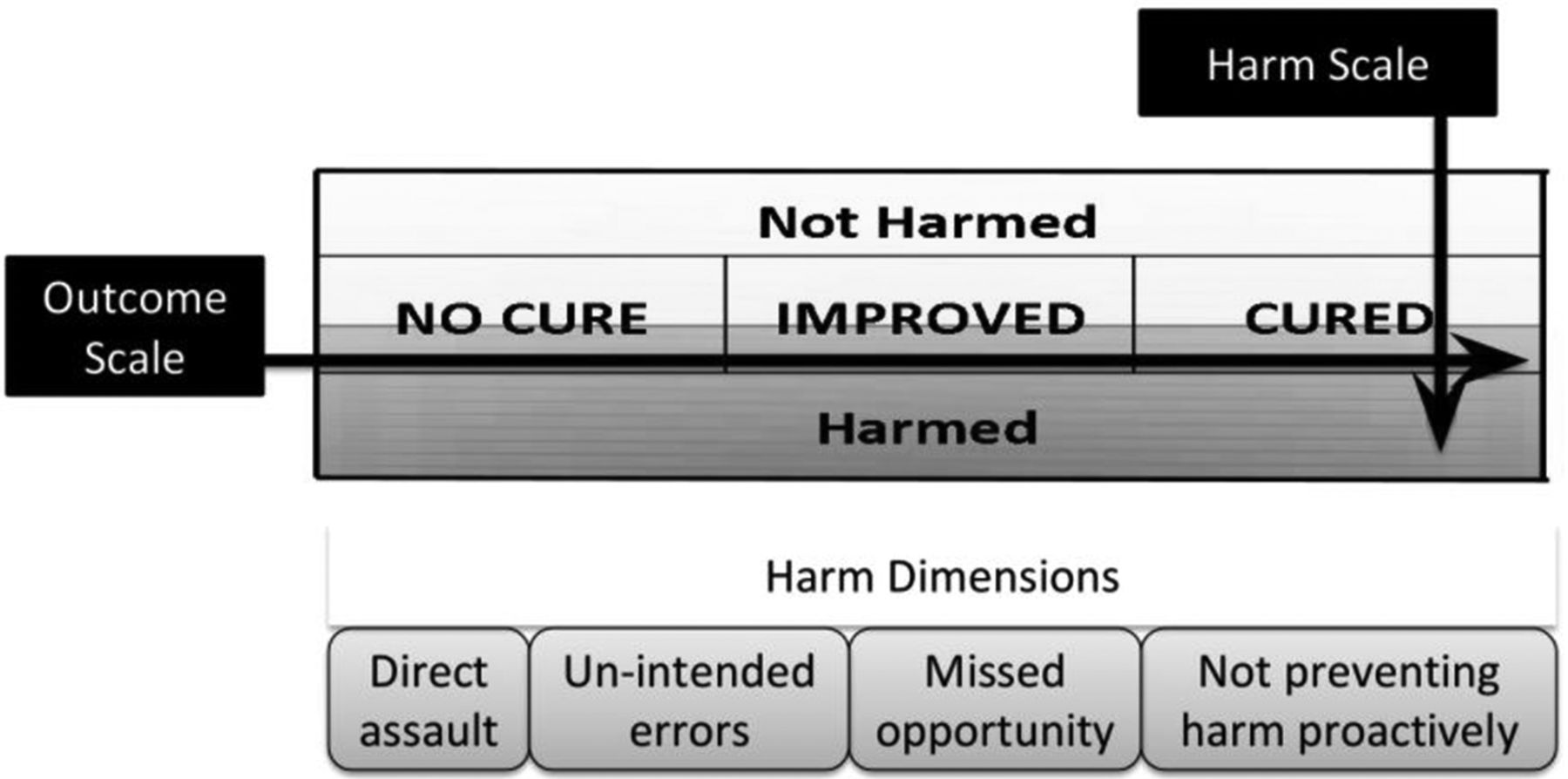
Learning to manage harms in healthcare is different because behavioural changes begin at the end of the spiral framework. The framework used to learn about harms is the reverse because it starts with an action, not a question, before evidence is collected to appraise or compare, which is similar to Costa and Kallick’s feedback spiral and recommendation for reflection on practice with a spiral approach.8 Data need to be collected to understand and compare actions and to understand causes before researching and experimenting the concluded evidence. The suggested spiral learning framework is the same as in figure 1, but reversed, so that the process is report/ask, collect data, assess, reflect/aggregate and implement evidence-based solutions. This approach to preventing harms is likely to facilitate improved efficiency in best-evidence practice. Additionally, figure 2 demonstrates the expression of harm, on a scale of low and high risk, and healthcare outcomes, on a scale of cured, improved or not cured, with different possible outcome combinations of both. The approach to improve quality or prevent harm should be targeted separately.
{kind=link}
{kind=link}
Dimensions of harm and its expression with outcome of care.
Managing harms has four dimensions (figure 2): active or intentional, such as unprivileged practices; errors implementing care, such as wrong site surgeries; omitting care, such as a predetermined protocol for myocardial infarction and not proactively preventing harm.
Learning environment
The learning environment must be directly targeted to promote spiral learning for evidence-based practice. It must be receptive to change. Learning in teams and through practice has been identified as important ways to develop HCP.9 Environments that promote a culture of continuous learning and quality improvements are equally important.
Conclusion
Teaching HCP how to make decisions and implement best practices requires a continuum of learning rather than one-time activities. Spiral learning should be applied to that continuum, and we should understand the crucial competencies throughout the process for reaching accurate answers and making appropriate decisions. Mastery of skills, knowledge and cognition that develop over time determines implementation of best evidence, which spiral learning emphasises. Employing this framework and learning the methodology will improve the implementation of best evidence in practice.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.