Article Text

Abstract
Although it is well established that cigarette smoking is associated with morbidity and mortality in several respiratory infections, data from recent studies suggest that active smokers are underrepresented among patients with COVID-19. This has led to claims that a ‘smoker’s paradox’ may exist in COVID-19, wherein smokers are protected from infection and severe complications of COVID-19. We aimed to review and summarise existing literature in this context. Electronic databases were searched for articles that reported prevalence of smokers among patients with COVID-19 or studied any association of smoking with outcomes among patients with COVID-19. We identified several biases and knowledge gaps which may give the false impression that smoking is protective in COVID-19. As of now, the data supporting smoker’s paradox claims are limited and questionable. Plausible biologic mechanisms by which smoking might be protective in COVID-19 include an anti-inflammatory effect of nicotine, a blunted immune response in smokers (reducing the risk of a cytokine storm in COVID-19) and increased nitric oxide in the respiratory tract (which may inhibit replication of SARS-CoV-2 and its entry into cells). On the other hand, smoking may worsen susceptibility and prognosis in COVID-19, in a manner similar to other respiratory infections. The claims of a protective effect must be viewed with extreme caution by both the general population as well as clinicians. Further investigations into the interaction between smoking and COVID-19 are warranted to accurately assess the risk of contracting COVID-19 among smokers, and progression to mechanical ventilation or death in patients suffering from it.
- coronavirus disease 2019
- COVID-19
- smoking
- nicotine
- tobacco
- outcomes
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
The relationship between smoking and coronavirus disease 2019 (COVID-19) has recently received a lot of attention. It is well established that cigarette smoking predisposes to several respiratory infections and is also associated with relatively poor outcomes in those suffering from these infections.1 Based on this knowledge, the World Health Organization (WHO) and the U.S. Food and Drug Administration (FDA) both released statements warning that smoking may increase the risk and severity of COVID-19.2 3 The assertion of risk associated with smoking, however, was rooted in expectation rather than data. Interestingly, recent studies have shown that active smokers are actually underrepresented among those requiring hospital treatment for COVID-19 in several countries including the USA, China and France.4 This led to widespread claims that smoking may be protective against COVID-19.4 5 Although a protective effect of smoking in COVID-19 may seem counterintuitive, researchers have suggested several mechanisms by which this ‘smoker’s paradox’ may be possible.4 In this article, we aim to (1) review currently available data regarding the relationship between smoking and COVID-19, (2) highlight possible biases in the available data and discuss current knowledge gaps, and (3) summarise proposed mechanisms of interaction between smoking and COVID-19.
Smoker’s paradox
The concept of ‘smoker’s paradox’ is not new. The term was first coined in 1995 to describe the unexpected favourable outcome of decreased short-term mortality in smokers after acute coronary syndrome6 7 and stroke,8 when compared with non-smokers. Conflicting theories exist in the literature, where some have proposed that this finding may be due to a decreased inflammatory response in smokers. Others suggest that this may be attributed to the difference in pathogenesis of myocardial infarction (MI) between the two groups, where a thrombotic MI occurring in smokers, compared with an atherosclerotic plaque-mediated event in non-smokers, would respond better to thrombolytic interventions.7 Another thought was that smokers may have ischaemic pre-conditioning, which would reduce infarct size. On the other hand, many simply attributed the apparently lower short-term mortality in smokers to differences in baseline characteristics between the two groups (such as younger age and fewer cardiovascular risk factors at the time of MI in smokers)9 or residual confounding by other factors (such as age at initiation of smoking)10 which are often not adequately adjusted for in observational studies.11 Of note, the majority of studies reporting this phenomenon group both current and former smokers under the common classification of ‘smoking’, despite smoking cessation showing a significant decrease in cardiovascular disease and subsequent mortality after a couple of years.12 Grouping both current and former smokers together can have potential confounding effects of nicotine withdrawal on the results, while excluding former smokers leads to ambiguity surrounding the existence of a smoker’s paradox in this subgroup.
A recent study on acute ST-elevation MI patients failed to confirm this hypothesised benefit of smoking, and instead showed worse outcomes in smokers after MI.13 Hence, the idea of a smoker’s paradox in cardiovascular disease has lost momentum in recent years. Given the recent claims that smoking has a protective effect in COVID-19, we must entertain the possibility of a smoker’s paradox in COVID-19. However, the experience with cardiovascular disease must be kept in mind, as many of the same biases may apply in the current situation.
Current evidence
The causal effects of smoking on disease processes have traditionally been difficult to study due to the impracticality of randomised controlled trials and a wide range of potential confounding factors. In such cases, causality is usually inferred via the process of triangulation, which involves using several research methods to study the same phenomenon. Thus, the same must be applied to study the relationship between smoking and COVID-19.
Search strategy and selection criteria of the reviewed studies
The PubMed and Scopus databases were searched in May 2020. Different combinations of following keywords and their MeSH terms were used: ‘Coronavirus disease 2019’, ‘COVID-19’, ‘characteristics’, ‘smoking’, ‘nicotine’ and ‘tobacco’. Bibliographies of included articles were also hand-searched for any articles that may have potentially been missed. In addition, a cursory search of pre-print servers was also performed for relevant articles with prominent results. Studies were included in this review if they reported smoking prevalence and/or its association with clinical outcomes in patients with diagnosed COVID-19. Studies reporting original data and systematic reviews/meta-analyses were considered. Table 1 summarises the characteristics of the studies reviewed for the purpose of this article. Furthermore, web searches (on www.google.co.uk) were conducted for relevant news articles and media reports.
Characteristics of studies reviewed
Prevalence of smokers among the COVID-19 population
The low prevalence of active smokers among hospitalised patients with COVID-19 has been a consistent finding across most published studies.14–21 A recent meta-analysis of 13 studies (n=5960 patients) demonstrated that the pooled prevalence of smokers among hospitalised patients with COVID-19 in China was 6.5% (95% CI 4.9% to 8.2%).22 This number is drastically lower than the prevalence of active smokers in the general population of China (26.6%).23 A recent study from France (currently available on a pre-print server) demonstrated a lower incidence of active smokers among 482 symptomatic patients with COVID-19, when compared with the general population.24 This French study included both inpatients and outpatients; thus, their results suggest that smokers may be less likely to be infected with COVID-19. Evidence from three published studies from the USA, all reporting data on hospitalised patients with COVID-19 in New York City, have reported different prevalence of active smokers. The prevalence of active smokers in the US population is 13.7%25; however, in the study by Goyal et al,26 smokers made up 20/393 (5.1%) of the hospitalised population. Cummings et al 27 reported an aggregated prevalence of current and former smokers in critically ill patients (33/257; 12.8%), which was also relatively low. The study by Richardson et al demonstrated a considerably higher prevalence (558/3567; 15.6%).28 To the best of our knowledge, the study by Richardson and colleagues is the only one to date in which the prevalence of smokers resembles that of the general population.
Association of smoking with clinical outcomes in COVID-19
Although smokers appear to be consistently underrepresented among patients with COVID-19, the link between smoking and clinical outcomes in these patients remains less clear. A systematic review, published in March 2020 by Vardavas and Nikitara,29 concluded that smoking was associated with disease progression and increased adverse outcomes in COVID-19; however, this conclusion was based on limited and mostly unadjusted data. In a meta-analysis published in the same time period, Lippi and Henry30 demonstrated no significant association between active smoking and COVID-19 severity (OR 1.69 (95% CI 0.41 to 6.92); p=0.254). The wide CIs derived in the meta-analysis are an indication of the heterogeneity of the studies and low reliability of the data. A large study of the general population of the UK found that smoking was significantly associated with increased COVID-19 mortality after age and sex adjustment (OR 1.25 (1.12 to 1.40)).31 However, after adjustment for multiple additional covariates, the same study found that smoking was associated with a reduced risk for COVID-19 mortality (OR 0.88 (0.79 to 0.99)). This protective association remained consistent after several individual adjustments to the model. Clearly, current evidence in the area is equivocal and limited, and further investigation is needed.
Limitations of current evidence
Several possible biases must be taken into consideration when assessing the current evidence in the area. First, several concerns have been raised regarding the quality of the data reported in published COVID-19 papers. Early in the pandemic crisis, there was a race to publish, which still continues to some extent. This likely resulted in aberrant and non-standardised data collection methods, poor statistical analysis, and limited scrutiny during editorial and peer review. In the context of smoking and COVID-19, poor data collection can lead to several erroneous conclusions. If patients with missing smoking data are not eliminated from the total pool, smokers may be wrongly underrepresented. Furthermore, it is difficult to get accurate history from patients who are either intubated or in respiratory failure. If data from these patients are missing, and these patients are not removed from the denominator, it can give a false impression that smokers are less likely to develop severe disease. Such errors are not far-fetched, especially when evaluating the effect of smoking is not the primary goal of the study. Second, it must be noted that most published studies have not reported the duration (years) or frequency (number of cigarettes) of smoking, hence these cannot be accounted for. Furthermore, most studies did not report the number of former smokers. It is conceivable that a proportion of the patients quit smoking only in the recent past (eg, after the start of the pandemic or after being diagnosed with COVID-19). As discussed earlier, inclusion of both former and current smokers as ‘smokers’ in these studies can create biases that contribute to smoker’s paradox. Third, none of the studies used objective biomarkers to determine active smoking. In fact, the source of smoking history in most published studies remains almost totally uncertain. Lastly, it must be kept in mind that the prevalence data in most studies are unadjusted. While using the general population as a control is convenient and offers some insight, the COVID-19 population likely has a different distribution of age, sex, comorbidities and smoking patterns.
Proposed interactions between smoking and COVID-19
Mechanisms by which smoking may have a protective effect
Despite all the aforementioned concerns with residual confounding, there are a few plausible biologic mechanisms by which smoking might indeed be associated with less severe COVID-19 disease. First, nicotine, which is an agonist of the cholinergic anti-inflammatory pathway, could potentially offer a protective effect in COVID-19.32 This is also a potential explanation for its ability to treat inflamed bowels. It inhibits production of pro-inflammatory cytokines such as TNF, IL-1 and IL-6, without inhibiting the anti-inflammatory cytokines such as IL-10,32 33 thereby possibly protecting against the cytokine-storm syndrome, a phenomenon responsible for the pathophysiology of severe COVID-19.34 Continuous suppression of these systemic cytokines in smokers may adapt their immune response in becoming more tolerant and therefore less reactive to the continuous inflammatory stimuli when compared with patients who have never smoked.35 Second, nitric oxide (NO) produced during smoking is involved in maintaining airway dilation and filtration prior to its entry in lungs.36 NO has been shown to inhibit the replication of SARS-CoV-2 and its entry into cells.37 Third, smoking may upregulate ACE2, an anti-inflammatory protein, in lower respiratory tract—as further discussed below (figure 1).
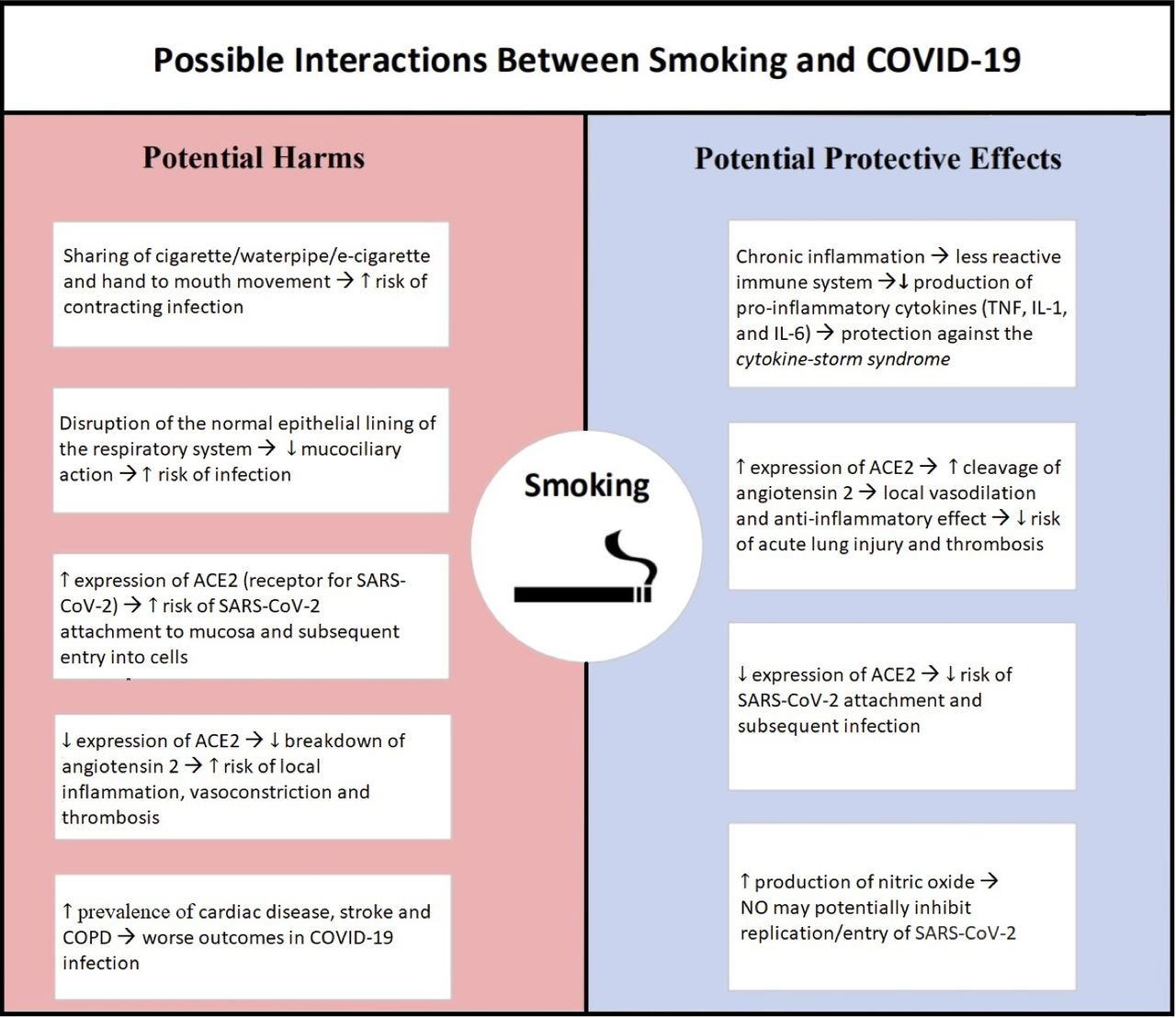
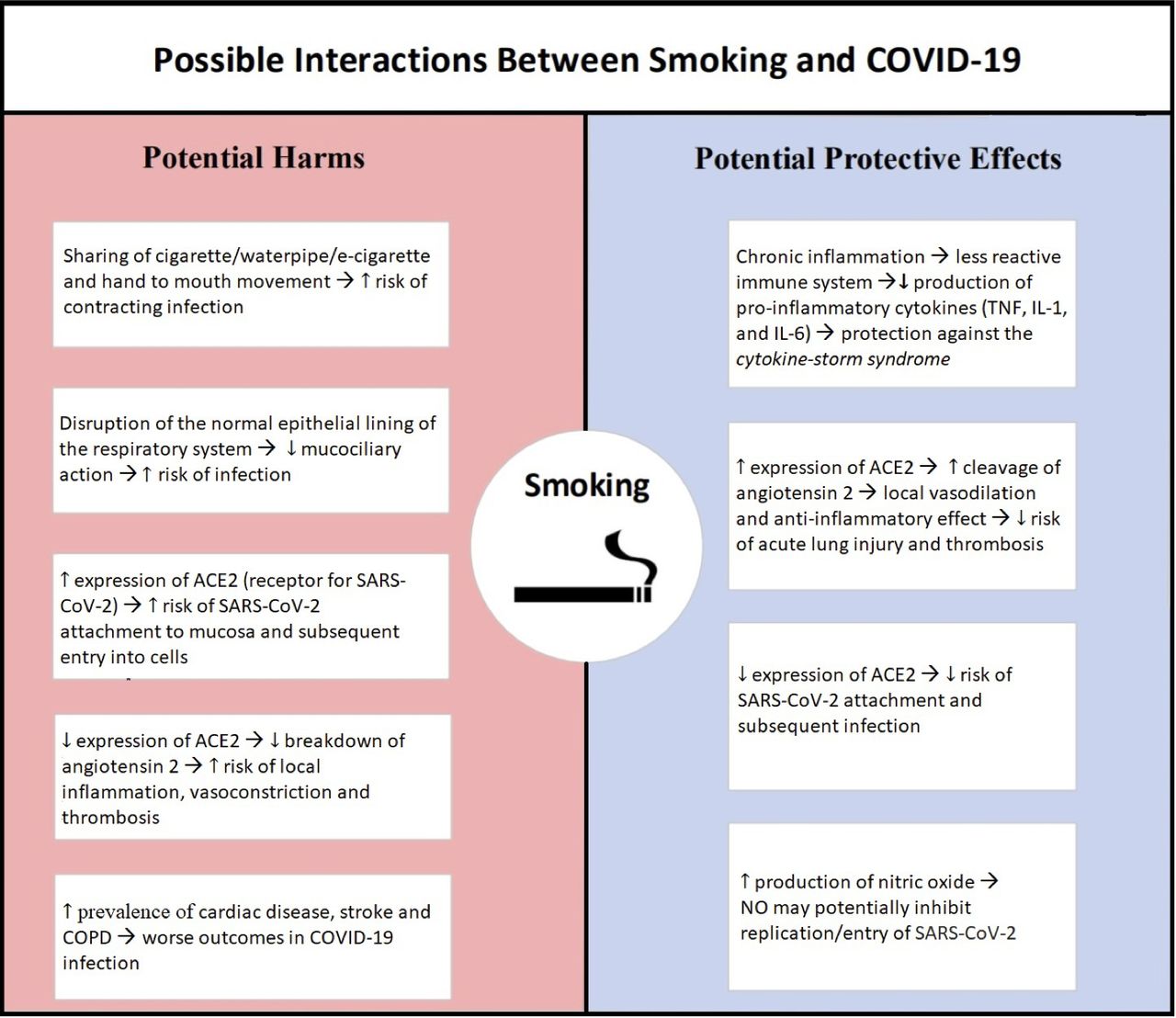{kind=link}
Proposed mechanisms of interaction between smoking and COVID-19. COPD, chronic obstructive pulmonary disease; ACE2, Angiotensin converting enzyme 2; IL-1, interleukin 1; IL-6, interleukin 6; NO, nitric oxide; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TNF, tumor necrosis factor
Mechanisms by which smoking may have a harmful effect
Smokers are almost certainly more vulnerable to initial exposure to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus responsible for COVID-19, due to repetitive hand-to-mouth movements and contact of possibly contaminated smoking apparatus with lips.38 Moreover, cigarettes are also sometimes shared between individuals. Patients may initially be asymptomatic, and such sharing may lead to inadvertent dissemination of the virus. Furthermore, smoking is a strong risk factor for premature cardiovascular diseases and chronic obstructive pulmonary disease, which have been shown to be associated with increased COVID-19 severity and mortality.39 40 Tobacco smoke suppresses the function of innate immune cells, including respiratory epithelium, alveolar surfactant, macrophage, neutrophils and lymphocytes. Tobacco contains components which disrupt the normal epithelial lining of the respiratory system leading to increased oxidative injury and impairment of mucociliary clearance.41 This may make smokers more susceptible to developing complications of COVID-19, such as pneumonia. Smoking also impairs production of surfactant, thereby leading to decreased leucocyte function and impaired host immunity.42 Moreover, the phagocytic function of alveolar macrophage is also significantly reduced by smoking, causing decreased clearance of inflammatory cells and debris from the lungs.43 Furthermore, cigarette smoking can also alter T-cell responses, which can lead to increased susceptibility to respiratory tract infections, which can be particularly detrimental in patients with concomitant COVID-19.43
Smoking and ACE2
ACE2, a cell surface protein expressed on several human tissues, is a known receptor for the SARS-CoV-2 virus. The physiological function of ACE2 is degradation of angiotensin II to angiotensin1–7, which serves as a protective function against overactivity of angiotensin II.44 In different experimental models, angiotensin II overactivity is reported to have triggered myocardial dysfunction, interstitial fibrosis, endothelial dysfunction, inflammation, oxidative stress and coagulation in addition to its primary function as a potent vasoconstrictor.45 On entering cells via ACE2, the virus then downregulates this protein.44 This prevents degradation of angiotensin II, and the subsequent local angiotensin II overactivity may be responsible for many of the inflammatory and thrombotic complications of COVID-19.44
Although it has been proposed that smoking modulates the expression of ACE2, the precise effect remains unclear. Recent literature reports that smoking and nicotine may upregulate ACE2,46 while studies published prior to the COVID-19 pandemic report smoking and nicotine to contribute to downregulation of ACE2.47 If smoking does in fact upregulate ACE2, then it may serve as a protective factor in decreasing disease severity. However if smoking diminishes ACE2 expression, further downregulation by SARS-CoV-2 virus may amplify the disease severity and promote adverse outcomes in this cohort.44 On the contrary, increased ACE2 receptors in smokers also potentially leads to increased viral receptors through which SARS-CoV-2 virus may enter the body.38 This contradiction warrants more research in order to most accurately determine the effect of nicotine on ACE2 expression and downstream consequences.
Conclusion
Although, on the surface, it appears that smokers are underrepresented among the COVID-19 population, we highlight several biases and knowledge gaps which have yet to be addressed. Currently reported data are questionable, and a protective effect should not be inferred. Claims that smoking is protective in COVID-19 can be detrimental to public health and should be viewed with extreme caution by both the general population as well as clinicians. Even if smoking did offer a protective effect in COVID-19, this is unlikely to outweigh the numerous proven adverse health effects of smoking. Hypotheses for both protective and detrimental effects of smoking on COVID-19 have been proposed in the literature (figure 1). Further investigation into the interaction between smoking and COVID-19 is warranted for two main reasons: (1) to assess the possibility of nicotine as a therapeutic option; (2) to allow accurate assessment of risk of contracting COVID-19 among smokers, and progression to mechanical ventilation or death in patients suffering from it.
Ethics statements
Patient consent for publication
Ethics approval
No human participants were involved in the study and it uses publicly available data.
References
Footnotes
Contributors MSU, TJS, AK and EDM contributed to conception of study and MSK and UKP contributed to study design. IS and JA contributed to literature search and MSU, TJS and MSK contributed to study selection. MSU, TJS, IS and JA contributed to initial manuscript draft. MSK, UKP, AK and EDM critically revised the manuscript for important intellectual content. MSU and TJS have contributed equally and are co-first authors. All authors have read and approved the final version of manuscript and agree to be accountable for accuracy and integrity of all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.