Article Text

Statistics from Altmetric.com
Haemorrhage is worldwide the leading cause of maternal death1 and an important cause of death after trauma.2 Antifibrinolytic drugs inhibit the lysis of a fibrin clot and are, therefore, used to stop or prevent haemorrhage. Intravenous administration of tranexamic acid has been shown to reduce the risk of death due to haemorrhage after trauma3 and the risk of death due to postpartum haemorrhage.4 Previous analyses have suggested that tranexamic acid needs to be administered early after the start of haemorrhage, because effects of delayed administration might be absent or even harmful for patients suffering life-threatening bleeding.3 4 A recent systematic review and individual patient-level data meta-analysis was set up to quantify the effect of treatment delay on the effectiveness of antifibrinolytics.5
This individual patient-level data meta-analysis was registered within PROSPERO and it adhered to the recognised protocols for systematic reviews and meta-analysis from The Cochrane Collaboration and the reporting guideline Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). It included randomised placebo-controlled trials (RCT) with more than 1000 patients with traumatic or postpartum haemorrhage; the authors argue that smaller studies have a lack of power and a risk of selection bias. The primary outcome for the meta-analysis was absence of death from bleeding. ‘Treatment delay’ was the exposure of interest and defined as the interval between bleeding onset and start of tranexamic acid treatment, or, if not available, as interval between birth and randomisation. The interaction between ‘treatment delay’ and treatment effect was examined in logistic regression models with absence of death from bleeding as the independent variable and various combinations of dependent variables: treatment, ‘treatment delay’ and its square, interaction terms for treatment with ‘treatment delay’ and its square, age, systolic blood pressure at randomisation and study.
Two RCTs randomising bleeding patients to tranexamic acid or placebo were included: the CRASH2 trial reporting on 20 211 bleeding trauma patients,3 and the WOMAN trial reporting on 20 060 women with postpartum haemorrhage.4 Any cause of death (primary outcome in original studies) and death from bleeding (primary outcome in the meta-analysis of the two studies) occurred in 15.2% and 5.3% in the CRASH2 and 2.4% and 1.7% in the WOMAN trial. The numbers needed to treat to prevent one death due to haemorrhage were 125 and 250 for patients with trauma and postpartum haemorrhage, respectively. The main result of the meta-analysis shows that the odds for absence of death from bleeding among patients treated with tranexamic acid compared with placebo was 1.72 (95% CI 1.42 to 2.10) among patients who had received tranexamic acid immediately, and it decreased by 10% for every 15 min of treatment delay.
This result is confounded by cause, severity and course of bleeding and it does not justify the interpretation of the authors. The authors concluded that a short delay in treatment reduces benefit of tranexamic acid administration and that all patients must be treated immediately. Yet, their results did not provide an estimate of the effect of earlier treatment of patients who were actually treated late (‘treating all patients immediately’).
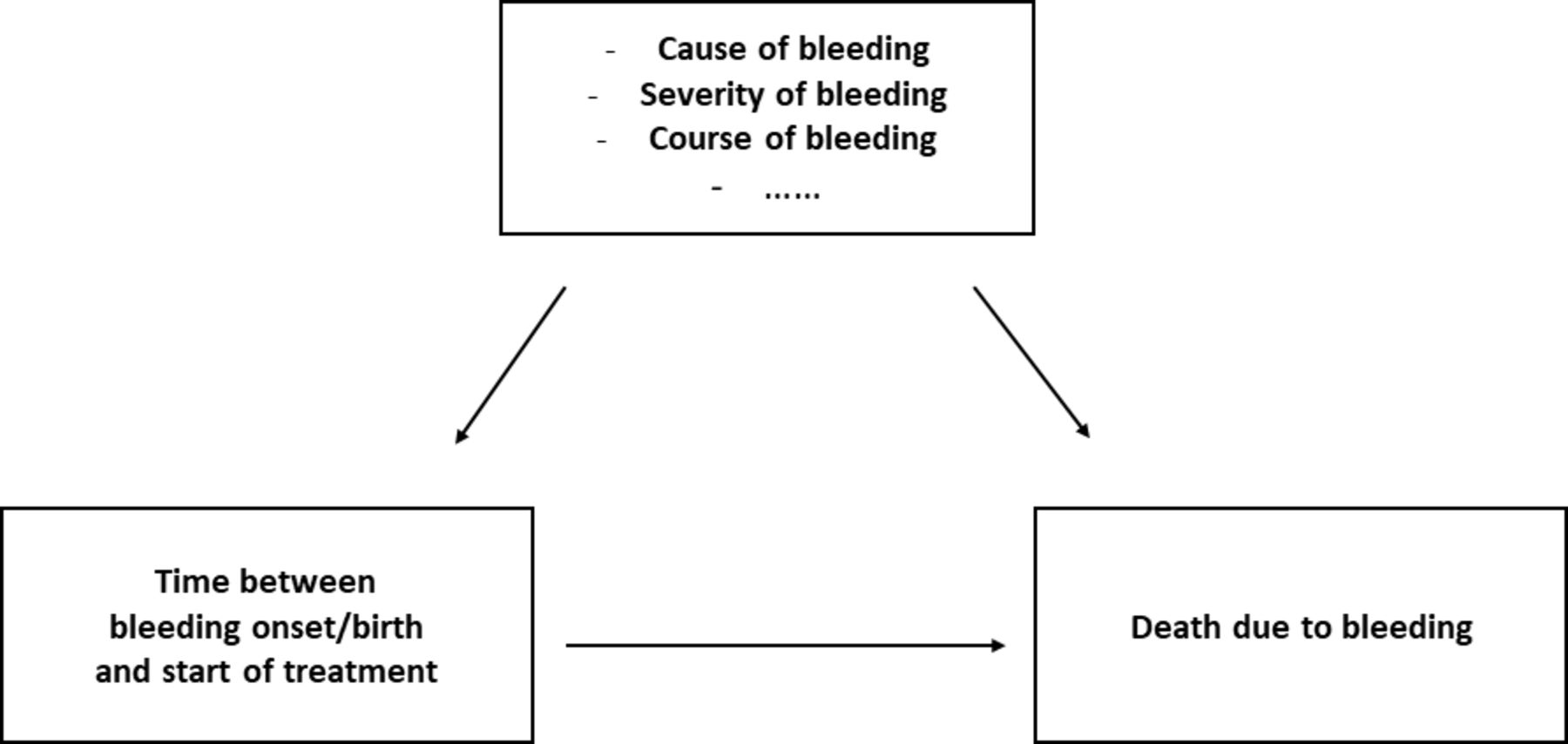
Patients who were randomised and treated late differ for several reasons from those who were randomised and treated earlier. Reasons for postponing randomisation (and administration of tranexamic acid) may have been: less severe bleeding, the clinical impression that the bleeding is about to stop or that the bleeding will stop due to other interventions. All these factors may influence the efficacy of treatment with tranexamic acid, and, therefore, also the findings. The authors acknowledge this bias and attempted to adjust for it by adding age and blood-pressure-at-inclusion into their regression model. One would need to adjust for many more variables to adequately correct for all the other potentially relevant differences between patients randomised at various times after the start of bleeding or after birth (figure 1).
{kind=link}
Causal graph illustrating that the causal association between the exposure ‘treatment delay’ and the outcome ‘death due to bleeding’ is confounded by cause, severity and course of bleeding. These confounders are time-dependent because of their change over time.
A better estimate of the effect of treatment delay on the effectiveness of tranexamic acid in patients with life-threating bleeding after trauma or childbirth would come from a study randomising patients to different treatment delays. However, such a trial is unethical given the evidence indicating that tranexamic acid may reduce haemorrhage related mortality.3 4 An observational study with adjustment for carefully measured time-dependent confounders may serve as an alternative, even though causal inference will remain difficult because of the risk of residual confounding due to unmeasured confounding variables. In this observational study, propensity score methods (ie, propensity score matching or inverse probability weighting) may be the best way to adjust for baseline and time-dependent confounders.6 7 A framework for this type of analysis in women with ongoing, severe postpartum haemorrhage was recently provided in a study on early timing of plasma transfusion to reduce maternal mortality and morbidity.8 In this study, propensity score matching was performed to adjust for the severity of bleeding at time of initiation of plasma transfusion. Severity of bleeding at the moment of initiation of plasma transfusions was expressed as volume of blood loss, bleeding rate and haemorrhagic shock. Severity of bleeding and all obstetric and haemostatic interventions performed before initiation of plasma transfusion were included in propensity scores to adjust for these time-dependent covariates.
Implications for practice
It is tempting to conclude that all patients with severe acute haemorrhage need to be treated as soon as possible after the start of the haemorrhage, but this conclusion is not supported by the findings of the meta-analysis. The findings show that the effect of tranexamic acid differs in subgroups of patients who were treated at different times after the start of bleeding. Future research should examine the underlying clinical characteristics that determine whether and when a patient with severe bleeding would benefit from treatment with tranexamic acid.
Ethics statements
Acknowledgments
We kindly thank R M Middelburg and R H H Groenwold for their critical appraisal of an earlier version of this commentary.
Footnotes
Contributors Both authors drafted and approve the contents of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.