Article Text

Abstract
Objectives To describe the development and initial evaluation of a brief e-learning course as a means of teaching shared decision making and risk communication skills to clinicians of all specialties.
Design Comparison pre-course and post-course of scores in subjective confidence and objective knowledge about shared decision making and risk communication.
Setting Online and open to all specialties and levels of clinical experience, including students.
Participants The course is freely available online and all who started the course from September 2018 to May 2020 were invited to participate in the evaluation study.
Intervention The self-guided e-learning course is made up of four modules and takes approximately 2 hours to complete. It is hosted on the website of the Winton Centre for Risk Communication and the UK’s National Health Service e-learning platform.
Main outcome measures Pre-course and post-course confidence in performing shared decision making (as measured by a 10-item scale adapted from the OPTION tool; total score range 10–50), and objective knowledge about basic principles of shared decision making and risk communication, as measured by performance on four knowledge questions and three calculations. At course commencement, a single item from the Berlin Numeracy Test, and the eight-item Subjective Numeracy Test were also asked.
Results Of 366 unique participants who consented and commenced the course, 210 completed all modules and the final post-course test. Participants’ mean age was 38.1 years, 69% were in current clinical practice and had a mean of 10.5 years of clinical practice. Numeracy was relatively low, with 50.7% correctly answering the Berlin Numeracy Test item pre-course. Participants who completed the course showed a significant improvement in their confidence by a mean summed score of 3.7 units (95% CI 2.9 to 4.6, p<0.0001) from a mean pre-course of 37.4 (SD 6.1) to post-course of 41.1 (SD 6.9). There was an increase in the proportion of correct answers for most knowledge questions (p<0.0001, p=0.013 for two directly compared), although no improvement in most skill questions that involved numbers (eg, calculating relative risks). Participants with higher numeracy appeared to show higher skill and confidence on most questions.
Conclusions This online, free e-learning course was successful in increasing participants’ confidence in, and some aspects of knowledge about, shared decision making and risk communication. It also highlighted the need for improvements in clinicians’ numerical skills as a vital part of training. We suggest that the course is used in combination with practical face-to-face experience and more intensive numerical skills training.
Data availability statement
Data are available in a public, open access repository. Anonymised data will be uploaded to an Open Science Framework repository on acceptance.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Most training opportunities for clinicians in shared decision making and risk communication are face-to-face workshops or not accessible for most clinicians.
What are the new findings?
A brief online e-learning course can improve clinicians’ knowledge and confidence in shared decision making, but in this study, little improvement in numerical tasks was demonstrated.
How might it impact clinical practice in the foreseeable future?
These freely available e-learning courses could be incorporated into clinical training at all levels to help improve clinicians’ knowledge and confidence in this area. Training to improve numeracy should also be included into curricula to enhance confidence and competence.
Introduction
Collaborative decision-making between clinicians and patients is an important component of contemporary, evidence-based healthcare. Shared decision making is a process that enables this and involves discussing the options; the pros and cons of these options, including the evidence-based estimates of benefits and harms for each (risk communication); and taking into account the patient’s values, preferences and circumstances.1 Shared decision making therefore relies on clinicians bringing together their skills in evidence-based practice and patient communication.2
There is an increasing expectation of greater collaborative decision-making in health decisions between clinicians and patients, with many health bodies and agencies around the world now mandating such collaboration (eg, see previous works3–6). The legal basis for informed consent in most countries now demands dialogue and risk communication personalised to the individual patient’s clinical and personal situation equally.7–9 However, shared decision making has not been routinely adopted by clinicians. Barriers to widespread implementation include clinicians not having sufficient knowledge about and skills in shared decision making,10 and believing that they are already undertaking it.1 11 Lack of opportunities for clinicians to be trained in shared decision making is also a barrier to its uptake.12
Most training opportunities are face-to-face workshops and courses that are available on occasion, to specific specialties or as part of research projects and these are not accessible to most clinicians, and very few formally and publicly evaluate their impact.13 An advantage of online courses is that they can be undertaken at a time and location convenient to busy clinicians or integrated into a medical curriculum for students in institutions where there may not be the resources or skills to teach the topic. The aim of this article is to describe the development and initial evaluation of a recently developed online course in shared decision making and risk communication, tailored to a broad range of health professionals and made freely available.
Methods
Participants
Eligible participants were users who undertook an e-learning course on shared decision making and risk communication and provided consent, at the course login page, for their responses to be analysed for this study. This occurred between September 2018 and May 2020.
Intervention
The e-learning course was originally developed by two of the authors (TH, CDM) in partnership with the Australian Commission on Safety and Quality in Healthcare. Iterative feedback was provided on drafts of the course by an advisory committee that consisted of representatives from various medical colleges. Versions of the course for UK clinicians were adapted by the Winton Centre for Risk Communication at the University of Cambridge with support from the Academy of Medical Royal Colleges (UK).
The course is free and open to anyone to undertake. It is hosted on the e-learning website of the Winton Centre for Risk Communication (https://moodle.wintoncentre.uk) and eLearning for Healthcare, the UK’s National Health Service (NHS) e-learning platform (https://www.e-lfh.org.uk/programmes/shared-decision-making/). It has been endorsed by the Academy of Medical Royal Colleges and accredited by relevant Royal Medical Colleges in the UK, including the Royal College of General Practitioners, the Royal College of Surgeons in England and the Royal College of Surgeons, Edinburgh, via newsletters, social media and website links.
Versions of the course have been created for different medical disciplines. There are five versions currently available: general practice, perioperative specialists (such as surgeons and anaesthetists), ophthalmologists, obstetricians and gynaecologists, and plastic surgeons. General content was common to each version; however, clinical scenarios and videos of demonstrated consultations were tailored to each discipline.
The course contains four parts, each commences with a list of learning objectives and concludes with list of relevant resources and further reading:
Part 1: Introduction to shared decision making and risk communication, the importance of these, how risk perception can affect behaviour, the need for accurate information about risks, introduction to absolute risks, relative risks, mortality rates and survival rates.
Part 2: Principles of shared decision making, what it is and what it is not, a model of shared decision making and its phases (3-talk model14), the relationship of shared decision making with motivational interviewing and informed consent, when it is and is not appropriate to undertake shared decision making, benefits of shared decision making, and inviting patients to participate in decision-making.
Part 3: Providing detailed information about options; considering benefits and harms; putting options into context and considering patients’ values and preferences; the role of decision support tools; resources for locating patient decision aids; risk communication, including probability and chance, risk perception, framing, words versus numbers to describe risk, communicating the risk of a single event, risk calculators, simple frequency and simple percentage format, absolute risk, communicating relative risk, absolute risk reduction, relative risk reduction, number needed to treat (NNT), baseline risk and communicating uncertainty.
Part 4: From preferences to decision; shared decision making and health literacy; communication skills and tools to help patients of all health literacy levels engage in decision-making; putting shared decision making into practice; and addressing some of the myths about shared decision making. This part ends with a multiple-choice self-test, including both the 10-item confidence questionnaire and a range of knowledge questions reprising the content of all four parts of the course.
In Part 1, participants are introduced to various patients and provided with basic demographic and clinical details and their reason for coming to a consultation (see figure 1). Throughout the course, these patients are used to illustrate the content that is covered, with videos of segments of consultations between the patient and a doctor. In the videos, actors were used as patients and doctors of the relevant disciplines volunteered to be video-recorded and were provided with a script which they could adapt to suit their natural style. Nine to 10 video clips are contained in each course. Most of them are very brief (eg, 20 s) and demonstrate the relevant element or step of shared decision making being taught. Towards the end of the course, there is a video of a consultation that demonstrates the entire shared decision making process.
Screenshots from the primary care version of the course.
The e-learning course is interactive and as part of the learning activities, participants complete knowledge and skills questions and are provided with immediate feedback and the correct answer. Most questions are forced-response. Some questions require a free-text response—these are not evaluated, but the elements of a model answer are provided after submitting a response to each question. At the end of the course there is a self-test section designed to test participants on key knowledge they should have gained during the course. All four modules in total take approximately 2 hours to complete.
Outcomes
In this evaluative study, we collected information on two aspects:
Confidence in knowledge and abilities
A set of questions about confidence in performing shared decision making behaviours were asked at the beginning and conclusion of the course. These questions were based on the 10 items adapted from the OPTION scale,15 with the stem question of “rate your confidence in the following…”.
Knowledge
We compared participants’ performance on the self-test questions at the end of the course with their previous answers to the same (or similar) questions which were embedded within the course. The questions embedded were all asked prior to any instruction in the relevant topic, designed to test the participants’ prior knowledge (and hence motivate their learning). These questions covered basic information about what shared decision making is and when it is appropriate; legal aspects of shared decision making and relationship with informed consent; the difference between mortality rates and survival rates; whether words can be used instead of numbers during risk communication; how to calculate absolute risk differences, relative risk differences and NNT and which to use when communicating with patients.
Demographic variables collected from participants were age, gender, level of education, medical specialty, number of years of clinical practice and level of any prior training in both shared decision-making and risk communication. Participants also completed the Subjective Numeracy Test16 (eight questions, answered with a Likert scale, regarding confidence using numbers in different contexts such as calculating a percentage discount off an item on sale when shopping) and for a subset of participants (those whose data were collected in the second year of the evaluation), we additionally measured their objective numeracy via a single question from the Berlin Numeracy Test17 (“Out of 1000 people in a small town 500 are members of a choir. Out of these 500 members in the choir 100 are men. Out of the 500 inhabitants that are not in the choir 300 are men. What is the probability that a randomly drawn man is a member of the choir? Please indicate the probability in percent.”) at the beginning of the course.
Data analysis
Data were collated from those who completed the courses on either of the two e-learning platforms hosting it and who consented for their responses to be used in this evaluation study. Responses to data were analysed descriptively. For the confidence questions, a paired t-test was used to compare pre-course and post-course summed scores within individuals. The association between explanatory variables (number of years of clinical experience, previous training in shared decision making, previous training in risk communication, or numeracy as measured by the single-measure question from the Berlin Numeracy Test) and post-course summed scores was assessed using analysis of covariance with adjustment for pre-course summed scores. McNemar’s test was used to compare the proportion of correct responses pre and post for the paired knowledge questions.
Ethics
This evaluation study was reviewed by the Psychology Research Ethics Committee at the University of Cambridge and granted approval (PRE.2018.034). All participants gave electronic informed consent to taking part in the evaluation.
Patient and public involvement
Patients and the public were not involved in the design or implementation of this study.
Results
Out of approximately 850 people who signed up to complete one of the courses during the evaluation period (duplicates not checked), 366 unique participants consented to be part of the evaluation (34 duplicates—people who had completed more than one version of the course—were removed). Of these, 313 started the course and 210 completed all four modules and all of the final self-test questions. The characteristics of participants are shown in table 1. The mean subjective numeracy score is 4.35 (SD 0.92), and the median is 4.5. Of the 133 who answered the objective numeracy question, 69 (50.7%) answered correctly.
Participant characteristics (n=366)
Confidence
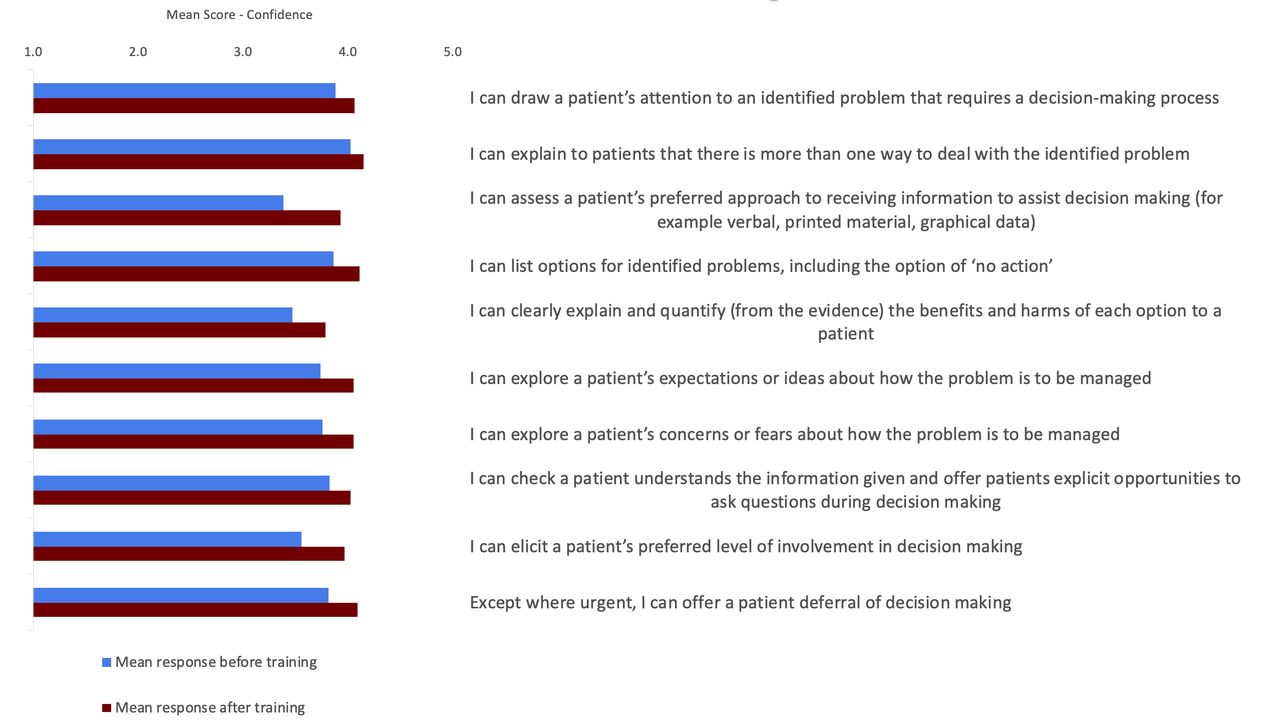
Figure 2 shows participants’ scores on each of the questions assessing confidence at the beginning and end of the course. There was an increase in mean summed score by 3.7 units (95% CI 2.9 to 4.6, p<0.0001, n=210) from pre-course to post-course (mean pre-course 37.4, SD 6.1; mean post-course 41.1, SD 6.9). The analysis of covariates showed that greater experience is associated with higher post-course summed scores by 0.09 units for each year of experience (95% CI 0.01 to 0.17, p=0.035); and an association between Berlin test and summed scores where a correct Berlin test response is associated with higher scores by 2.7 units on average (95% CI 0.9 to 4.6, p=0.003). There was no association between previous training in either shared decision making or risk communication and post-course summed scores (shared decision making: effect on score 0.17, 95% CI −1.4 to 1.8, p=0.82; risk communication: effect on score −0.18, 95% CI −1.8 to 1.4, p=0.80).

{kind=link}
{kind=link}
Mean scores, at the beginning and end of the course, for each confidence item.
Knowledge
Knowledge: questions asked once
As part of the course, participants complete questions and are provided with immediate feedback and the correct answer. Questions are asked before the content is covered as a lead into the content. Many of these questions are not repeated, and some are not strictly relevant in assessing clinician’s knowledge of the topic, however, they are presented in table 2 to give an indication of participants’ level of knowledge in this area. At the end of the final module of the course, there is a self-test quiz which reprised several of the key questions, or variations on them, as an indication of knowledge gained. This was designed both as a self-test for participants and as a part of the evaluation study.
Percentage of correct responses to shared decision making and risk communication knowledge questions (in the course before content covered and at the end)
With questions involving some arithmetic (such as calculating absolute and relative risks, and NNT), those with higher numeracy outperformed those with lower numeracy on each question. However, even those with higher numeracy performed less well on the calculation questions than on factual knowledge.
Knowledge: pre-course and post-course
In table 2, superscript letters mark similar questions that were asked both pre-course and post-course. Participants’ knowledge about mortality versus 5-year survival rates showed no change (p=0.09, McNemar’s test), but knowledge about documentation of shared decision making (p=0.013) and whether verbal terms are a good alternative to numbers in communicating risk (p<0.0001) increased. Overall, participants’ factual, non-numerical knowledge was at a high level (>85% correct) after the course, apart from two questions (‘SDM is a legal necessity as part of informed consent: true or false?’, with 54% answering correctly and ‘When communicating risks to be compared, it is best to communicate in the format ‘one in x people are likely to experience…’ (eg, 1 in 10 compared with 1 in 250) rather than keeping the denominator the same (eg, 100 in 1000 compared with 4 in 1000)?’ with 68% answering correctly). The proportion of correct responses for the numerical questions (both those that required calculations and those about understanding numbers) showed no significant change from pre-course to post-course, with about half responding correctly to such questions throughout.
Discussion
Completing a brief (approximately 2 hours) online course in shared decision making and risk communication appeared to affect participants in several ways. First, it increased their confidence in their abilities to facilitate shared decision making and communicate risks. Those with more clinical experience and higher numeracy had higher confidence in their abilities. Second, it increased participants’ knowledge about some of the basic principles of shared decision making and risk communication, and by the end of the course, participants’ knowledge about basic concepts was at a good level, with over 85% answering correctly on all but two questions. Third, however, it did not appear to help people consistently better calculate or interpret the statistical elements of risk communication.
Participants with higher numeracy performed better than those with lower numeracy on numerical questions, but many appeared to struggle with the concept of lead-time bias, and with the calculation of relative risks or NNT. In the pre-course question, relative risk increase was given as part of the question text, but even so only just over half of participants correctly recognised it. In the post-course test, two questions required calculations—one presenting the original numbers as frequencies and the other as percentages. Converting from frequencies into percentages (especially as the frequencies were not ‘out of 100’) seemed to cause difficulties, with only about a quarter of participants being able to say that a relative risk increase from 1 to 5 was 500%.
Comparison with other studies
Few studies assessing shared decision making training programmes have evaluated the impact of training on participants’ confidence and knowledge.18 An 8-hour face-to-face training programme for physicians reported an increase in confidence and knowledge, but areas of knowledge assessed are not detailed.19 Evaluation of a brief online single case-based approach for primary care clinicians reported a reasonable level of confidence in performing and high level of knowledge of shared decision making steps after completing the case, but levels were not measured prior to undertaking it.20 The online Ottawa Decision Support Tutorial,21 which has shown to increase participants’ shared decision making skills when combined with face-to-face training (eg, previous work22), does not include risk communication components. Other online courses for shared decision making are designed to train clinicians in specific clinical areas, such as diabetes care23 or prostate cancer screening.24 25 A study evaluating the eDoctoring platform26 (now technologically out of date as it requires Flash software), which had a shared decision making module as part of its online teaching of genetic counselling, found no increase in shared decision making knowledge scores, but an increase in behaviours in the clinic.27 It is not clear whether this course included risk communication, and this component of training was particularly noted as lacking across all courses in the review of shared decision making training interventions by Coates and Clerke.18 There are few online courses that have been evaluated or published results. While face-to-face training has been shown to increase knowledge and confidence in shared decision making, uptake of such training is greatly restricted by limitations in its accessibility.
Performance on the single objective numeracy question, with 50.7% (n=133) answering correctly, is higher than the 23% of those with a bachelors’ degree or above (n=262) answering the question correctly in a recent survey of a UK population (representative by age and gender) carried out by one of the authors (unpublished data), and 38% (n=175) in a survey of surgeons from developed countries.28
Strengths and weaknesses
The sample in this study consisted of a broad range of health professionals, from medical students to experienced clinicians from a variety of specialties. The sample size is also large compared with other studies of this type. All participants were completing the course under real-life conditions rather than as a laboratory-style controlled study, and the intervention—the e-learning course—is available freely online for use by medical schools, professional bodies, and clinicians at any time.
A weakness is that participants who opted to take part in the evaluation study were a minority of those undertaking the course and a self-selected group. There was also considerable attrition across the course, with a possible further bias in those who completed the whole course so these results cannot be taken as representative of participants in general. Subgroup analyses (such as those for high/low numeracy participants) are based on small numbers and must be considered only suggestive of patterns.
The self-test questions that form the ‘post-course’ test were at the end of an approximately 30 min module, and participant motivation and effort may have been lower than during pre-course tests at the start of individual modules, thus a potential contributory factor to poor performance on questions that required calculations or contemplation. The knowledge questions were not designed for an evaluative study, but as learning activities as part of the modules, and some of the paired questions are not identical from pretest to post-test. This was not possible as immediate feedback and the correct answer was provided as participants progressed through the course.
Meaning of the study
Confident shared decision making and good risk communication with patients is ultimately a skill that needs practice and cannot be learnt solely through theoretical knowledge and watching others. However, this evaluation shows that an e-learning course can help clinicians understand some of the theoretical underpinnings of shared decision making and risk communication and increase their confidence in being able to incorporate these skills into clinical practice. Both of these are valuable precursors to a full face-to-face course in shared decision making, including practice with (simulated) patients as improved confidence and knowledge are not necessarily enough for clinicians to carry the skills into their practice. While training is an important first step towards shared decision making uptake, previous experience shows that clinicians also need opportunities to practise and develop their skills, an appropriate attitude, and a supportive organisational culture to assist with the implementation of shared decision making.11 29
This study also raises once again the issue of clinician numeracy. The poor performance of the participants throughout the study on questions that involved simple arithmetic (such as calculation of the absolute difference between two numbers) is worrying. Lower numeracy was also associated with lower confidence ratings on the post-course assessment. Although motivation to put thought into answers may be low during the e-learning course (where marks carried no consequences for the participants), clinicians who cannot easily do these sorts of calculations are unlikely to be able to accurately interpret or clearly communicate them to patients in real consultations\.
While this is a problem that has been raised many times before (eg, see previous works28 30–34), poor numeracy has been linked to poor decision-making ability in a number of scenarios (eg, see previous work35–39) and this study again raises the need to support clinicians further during and after their training to increase their skills and confidence when dealing with numbers. Additionally, ensuring that decision support tools are designed to communicate numbers simply, so that they are appropriate for use with both clinicians and patients regardless of numeracy level, is important. A recent study of risk communication training in a medical school in Germany highlighted the lack of teaching there,40 and effective—but intensive—courses have been developed elsewhere (eg, see previous works41–43). These require many hours of face-to-face teaching, which is impractical for many medical schools to deliver and for clinicians to access. Our study shows that an e-learning course has the potential to increase understanding of and confidence in shared decision making—but that it needs to incorporate, or be accompanied by, more support around the numerical concepts and skills required for good interpretation of numerical evidence and risk communication.
Unanswered questions and future research
While we are hopeful that the increased confidence and knowledge of the importance of shared decision-making demonstrated by participants on completion of this e-learning course will translate to application of it in clinical practice, this remains to be demonstrated. It is also unclear how much participants’ risk communication skills increased due to limitations in their numeracy. A study assessing participants’ actual performance of shared decision making and risk communication in clinical practice before and after taking the online training may help to highlight what tools, training and other supports could best accompany the current e-learning course.
It is also clearly vital to work on ways to improve participants’ numerical skills and risk communication. This could potentially be done through e-learning courses, such as spending more time on the numerical aspects in this course, as it is a skill that can be practised by individuals on their own. However, numerical training should also be a core part of face-to-face teaching and examination as part of medical curricula given its demonstrably important role in clinician confidence and competence. In addition, graphical aids designed to support people with a range of numeracy levels in clinical situations could help clinicians who lack confidence with numbers to deal with the communication of risk information.44 45
Conclusions
This free e-learning course helps clinicians understand the principles and concepts of shared decision making and risk communication, and increases their confidence in being able to carry it out. However, clinician numeracy is worryingly low and a barrier to good risk communication. Both undergraduate curriculum and continuing medical education need to effectively teach knowledge and skills in evidence-based medicine, shared decision making and risk communication, with clear articulation of the interface and interdependence between these areas.
Data availability statement
Data are available in a public, open access repository. Anonymised data will be uploaded to an Open Science Framework repository on acceptance.
Ethics statements
Patient consent for publication
Ethics approval
This evaluation study was reviewed by the Psychology Research Ethics Committee at the University of Cambridge and granted approval (PRE.2018.034).
Acknowledgments
We thank Associate Professor Mark Jones for assistance with statistical analysis and Dr Elizabeth Gibson for assistance with data preparation. We would also like to thank all the participants who opted to take part in this evaluation study.
References
Footnotes
Contributors TCH and CDM developed the original course, which was modified for the UK audience by AF with support and national endorsement from RS. AF collected and cleaned the evaluation data, which was analysed by TH. TCH, AF and CDM drafted the manuscript. The corresponding author acts as the guarantor and attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted, and that the manuscript represents an honest, accurate and transparent account of the study with no important aspects having been omitted.
Funding The development of the original e-learning course was funded by the Australian Commission on Safety and Quality in Health CareHealthcare and is used under license by the Academy of Medical Royal Colleges. The adaptations for the UK and different specialties was funded by the Winton Centre for Risk and Evidence Communication at the University of Cambridge, which is itself funded by a donation from the David & Claudia Harding Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.