
Effect of Smoking Reduction Therapy on Smoking Cessation for Smokers without an Intention to Quit: An Updated Systematic Review and Meta-Analysis of Randomized Controlled

Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
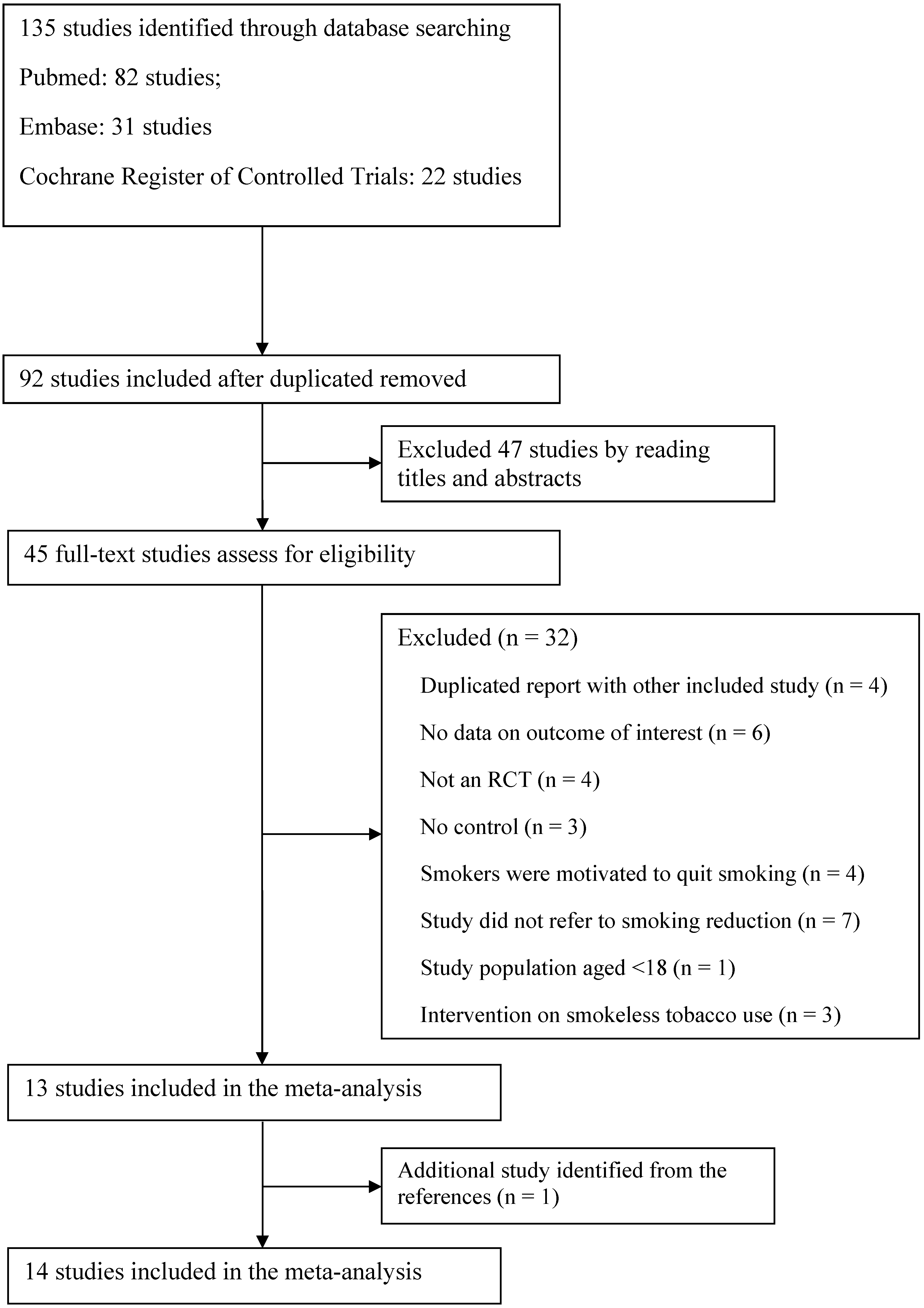
3.1. Study Identification and Selection
3.2. Study Characteristics

3.3. Quality Assessment
3.4. Primary Outcome
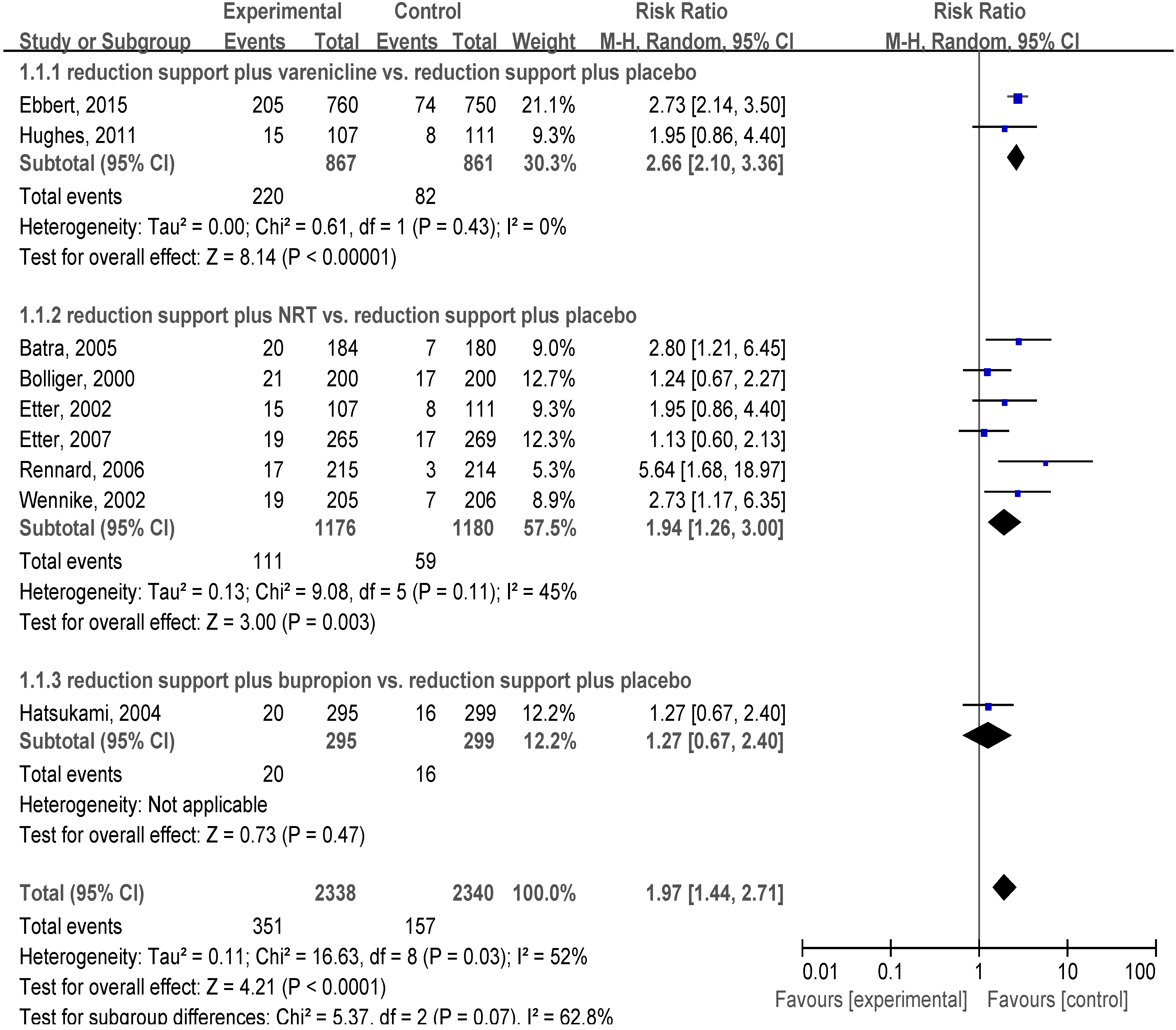
3.4.1. Reduction Support Plus Medication vs. Reduction Support Plus Placebo
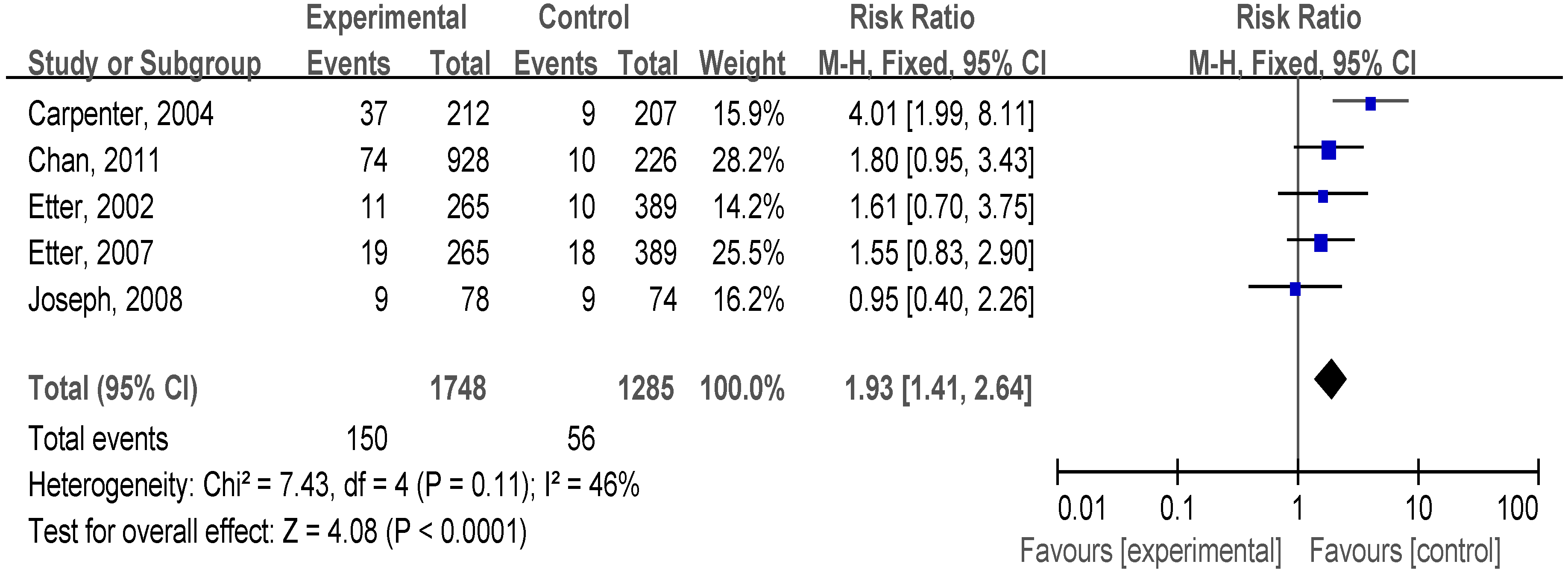
3.4.2. Reduction Support Plus Medication vs. no Intervention

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Sample Size | Design | Setting | Initial Intention to Quit | Population | Male N (%) | Age (Years) Mean (SD) | Cigarettes/Day Mean (SD) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Treat Control | Treat Control | Treat Control | |||||||||
| Bolliger, 2000 [18] | 400 | multi-centre | Switzerland | willing to reduce their smoking but unable or unwilling to stop smoking immediately | healthy | 104 (52.0) | 86 (43.0) | 45.8 (10.5) | 46.4 (10.5) | 30.3 (12.1) | 28.2 (11.4) |
| Batra, 2005 [19] | 364 | multi-centre | Switzerland | willing to change their smoking behavior but unwilling to quit | healthy | 101 (54.1) | 117 (64.8) | 42.6 (9.9) | 43.5 (10.3) | 27.9 (9.2) | 29.6 (9.5) |
| Carpenter, 2003 [20] | 67 | single-centre | United States | no interest in quitting smoking in the next 30 days | healthy | 26 (74.3) | 20 (62.5) | 43 (12) | 44 (9) | 24 (10) | 23 (10) |
| Carpenter, 2004 [21] | 616 | single-centre | United States | did not wish to quit | healthy | 144 (67.9) | 123 (62.4) 139 (67.1) | 38 (12) | 39 (13) 41 (14) | 23 (10) | 21 (8) 22 (9) |
| Chan, 2011 [22] | 1154 | single-centre | Hong Kong | no intention to quit in the near future but interested in reducing smoking | healthy | 748 (80.6) | 198 (87.6) | 41.9 (10.3) | 42.5 (11.2) | 19.9 (9.8) | 19.2 (8.9) |
| Etter, 2002 [23] | 923 | single-centre | Switzerland | no intention to quit smoking in the next 6 months | healthy | 143 (54.0) | 132 (49.0) 171 (44.0) | 43.2 | 41.7 42.9 | 29.8 (10.3) | 29.4 (9.4) 30.2 (10.4) |
| Etter, 2007 [24] | 923 | single-centre | Switzerland | no intention of quitting smoking in the next 6 months | healthy | 54 (20.4) | 49 (18.2) 44 (11.3) | 43.2 | 41.7 42.9 | 29.8 (10.3) | 29.4 (9.4) 30.2 (10.4) |
| Ebbert, 2015 [25] | 1410 | multi-centre | 10 countries | not willing or able to quit smoking within the next month but willing to reduce smoking and make a quit attempt within the next 3 months | healthy | 425 (55.9) | 426 (56.8) | 44.7 (11.8) | 44.4 (12.0) | 20.6 (8.5) | 20.8 (8.2) |
| Glasgow, 2009 [26] | 320 | single-centre | United States | not interested in quitting smoking at that time | healthy | 44 (26.8) | 44 (28.2) | 54.8 (10.4) | 56.0 (11.3) | 21.2 (9.4) | 20.1 (9.0) |
| Hatsukami, 2004 [27] | 594 | multi-centre | United States | motivated to reduce their cigarette usage, but who were unwilling or perceived themselves to be unable to quit smoking at the time of screening | healthy | 169 (57.3) | 158 (52.8) | 42.5 (11.0) | 42.0 (11.6) | 29.0 (9.8) | 28.5 (9.6) |
| Hughes, 2011 [28] | 218 | multi-centre | United States | interested in quitting but had no plans to quit in the next month | healthy | 65 (60.7) | 63 (56.8) | 44 (14) | 41 (15) | 19 (9) | 17 (7) |
| Joseph, 2008 [29] | 152 | multi-centre | United States | unwilling or uninterested in setting a stop smoking date in the next 30 days | cardiovascular patient | 70 (89.7) | 65 (87.8) | 57.5 (8.6) | 58.4 (9.6) | 27.7 (12.5) | 27.0 (11.0) |
| Rennard, 2006 [30] | 429 | multi-centre | United States | did not plan to quit smoking within the next 4 weeks, but want to reduce cigarette consumption | healthy | 88 (40.9) | 104 (48.6) | 45.9 (12.3) | 44.8 (12.1) | 29.3 (10.1) | 30.4 (9.9) |
| Wennike, 2002 [31] | 411 | single-centre | Denmark | unwilling or unable to quit smoking, but interested in reducing their smoking | healthy | 72 (35.0) | 85 (41.0) | 45 (10) | 44 (10) | 24 (7) | 24 (7) |
| Trial | Treat vs. Control | Treatment Duration (Months) | Follow-up (Months) | Carbon Monoxide-Confirmed | Outcome | Quit Rate | |
|---|---|---|---|---|---|---|---|
| Treat/Total N (%) | Control/Total N (%) | ||||||
| Reduction support plus medication versus reduction support plus placebo | |||||||
| Bolliger, 2000 [18] | nicotine inhaler plus reduction counseling vs. placebo inhaler plus reduction counseling | 18 | 24 | Yes | 7-day point | 21/200 (10.5) | 17/200 (8.5) |
| Batra, 2005 [19] | 4-mg nicotine gum plus reduction counseling vs. placebo gum plus reduction counseling | 12 | 13 | Yes | 7-day point | 20/184 (10.9) | 7/180 (3.9) |
| Etter, 2002 [23] | NRT (gum, inhaler or patch) plus reduction booklet vs. placebo plus reduction booklet | 6 | 6 | No | sustained for 4 weeks | 11/265 (4.2) | 5/269 (1.9) |
| Etter, 2007 [24] | NRT (gum, inhaler or patch) plus self-help reduction material vs. matching placebo plus self-help reduction material | 6 | 60 | No | sustained for 60 months | 19/265 (7.2) | 17/269 (6.3) |
| Ebbert, 2015 [25] | Varenicline plus four brief reduction counseling vs. placebo plus four brief reduction counseling | 6 | 12 | Yes | sustained (week 21 to 52) | 205/760 (27.0) | 74/750 (9.9) |
| Hatsukami, 2004 [27] | bupropion plus reduction counseling vs. placebo plus reduction counseling | 12 | 12 | Yes | sustained (week 4 to 26) | 20/295 (6.8) | 16/299 (5.4) |
| Hughes, 2011 [28] | Varenicline plus four brief reduction counseling vs. placebo plus four brief reduction counseling | 2 (4) | 6 | Yes | 7-day point | 15/107 (14.0) | 8/111 (7.2) |
| Rennard, 2006 [30] | 10-mg nicotine inhaler plus reduction counseling vs. placebo inhaler plus reduction counseling | 12 | 15 | Yes | 7-day point | 17/215 (7.9) | 3/214 (1.4) |
| Wennike, 2002 [31] | nicotine gum plus reduction counseling vs. placebo gum plus reduction counseling | 12 | 24 | Yes | 7-day point | 19/205 (9.3) | 7/206 (3.4) |
| Reduction support plus medication versus no intervention | |||||||
| Carpenter, 2004 [21] | telephone-based reduction counseling plus NRT (gum or patch) plus brief advice vs. no intervention | 6 | 6 | No | 7-day point | 37/212 (17.5) | 9/207 (4.3) |
| Chan, 2011 [22] | NRT plus 4 brief reduction counseling vs. simple advices | 6 | 6 | Yes | 7-day point | 74/928 (8.0) | 10/226 (4.4) |
| Etter, 2002 [23] | NRT (gum, inhaler or patch) plus reduction booklet vs. no intervention | − | − | − | − | 11/265 (4.2) | 10/389 (2.6 |
| Etter, 2007 [24] | NRT (gum, inhaler or patch) plus reduction material vs. no treatment | − | − | − | − | 19/265 (7.2) | 18/389 (4.6) |
| Joseph, 2008 [29] | NRT (gum or patch) plus reduction counseling vs. no intervention | 18 | 18 | No | 7-day point | 9/78 (11.5) | 9/74 (12.2) |
| Reduction support plus medication versus other support plus medication | |||||||
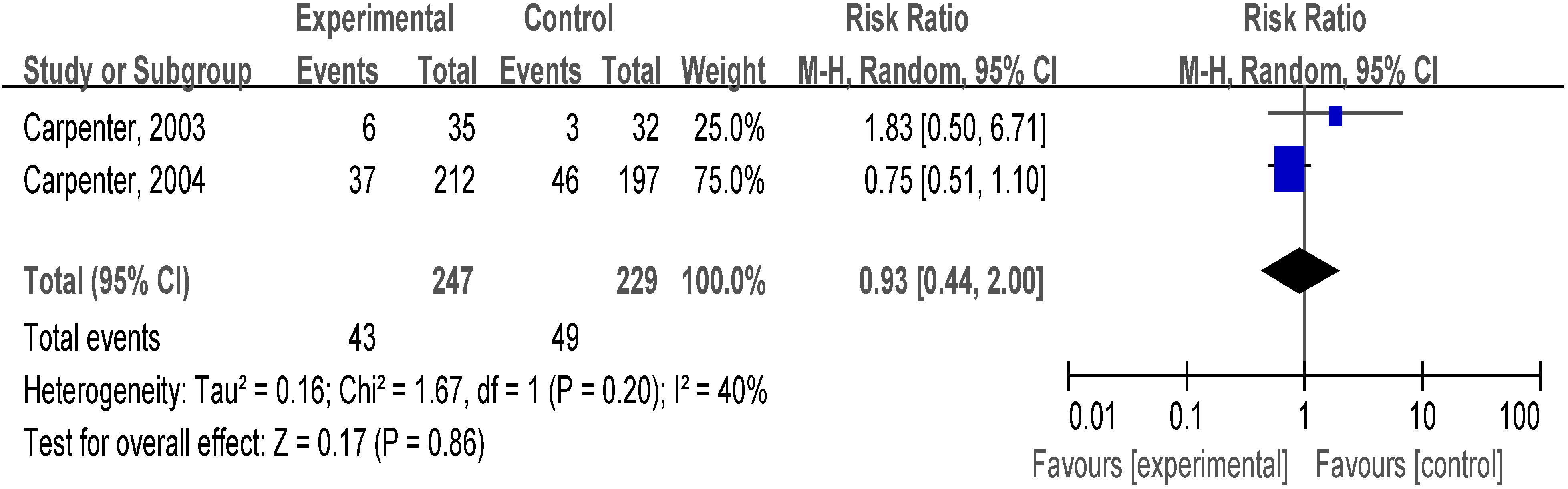
| Carpenter, 2003 [20] | NRT (gum, inhaler or patch) plus reduction counseling vs. NRT plus brief advice | 6 | 6 | Yes | 7-day point | 6/35 (17.1) | 3/32 (9.4) |
| Carpenter, 2004 [21] | telephone-based reduction counseling plus NRT (gum or patch) plus brief advice vs. motivational advice plus NRT for quit attempt plus brief advice | − | − | − | − | 37/212 (17.5) | 46/197 (23.4) |
| Reduction support versus no intervention | |||||||
| Glasgow, 2009 [26] | behavioral reduction supports vs. no intervention | 12 | 12 | Yes | 7-day point | 11/164 (6.7) | 7/156 (4.5) |


3.4.3. Reduction Support Plus Medication vs. other Support Plus Medication
3.4.4. Reduction Support vs. No Intervention

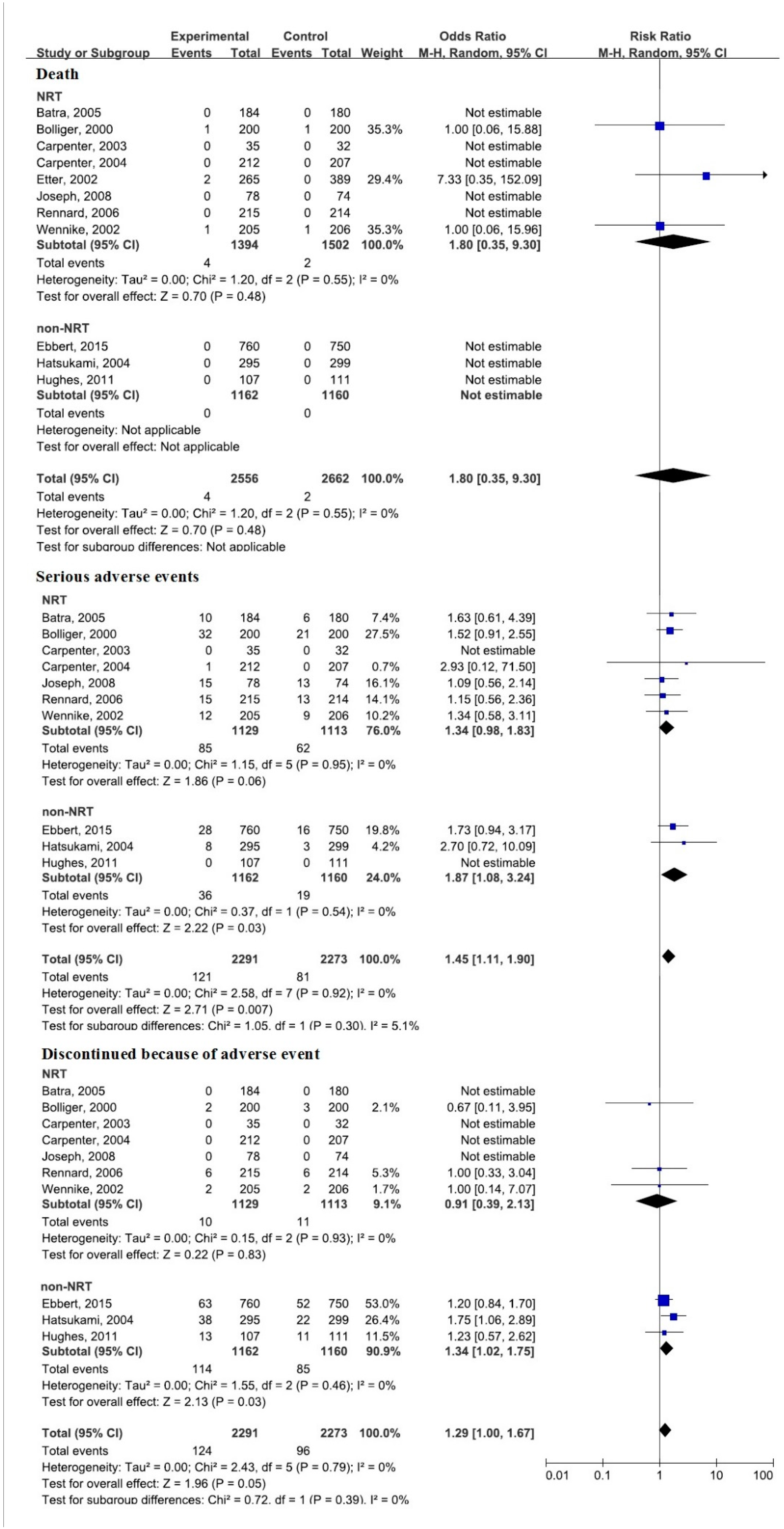
3.5. Secondary Outcomes
3.6. Sensitivity Analysis

3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Author Contributions
Conflicts of Interest
Abbreviations
| CENTRAL | Cochrane Central Register of Controlled Trials |
| RCT | randomized controlled trial |
| RR | relative risk |
| 95% CI | 95% confidence interval |
| NRT | nicotine replacement therapy |
References
- Jiang, Y.; Elton-Marshall, T.; Fong, G.T.; Li, Q. Quitting smoking in China: Findings from the ITC China Survey. Tob. Control 2010, 19, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.; Gandini, S.; Robertson, C. Characteristics of smokers’ attitudes towards stopping: Survey of 10,295 smokers in representative samples from 17 European countries. Eur. J. Public Health 2000, 10, 5–14. [Google Scholar] [CrossRef]
- Jamal, A.; Agaku, I.T.; O’Connor, E.; King, B.A.; Kenemer, J.B.; Neff, L. Current cigarette smoking among adults—United States, 2005–2013. Morb. Mortal. Wkly. Rep. 2014, 6, 1108–1112. [Google Scholar]
- Hughes, J.R.; Carpenter, M.J. The feasibility of smoking reduction: An update. Addiction 2005, 100, 1074–1089. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.S. How far should we promote smoking reduction in order to promote smoking cessation? Asian Pac. J. Cancer Prev. 2005, 6, 231–234. [Google Scholar] [PubMed]
- Glasgow, R.E.; Morray, K.; Lichtenstein, E. Controlled smoking vs. abstinence as a treatment goal: The hopes and fears may be unfounded. Behav. Ther. 1989, 20, 77–91. [Google Scholar] [CrossRef]
- Hughes, J.R.; Carpenter, M.J. Does smoking reduction increase future cessation and decrease disease risk? A qualitative review. Nicotine Tob. Res. 2006, 8, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.; Aveyard, P.; Connock, M.; Wang, D.; Fry-Smith, A.; Barton, P. Effectiveness and safety of nicotine replacement therapy assisted reduction to stop smoking: Systematic review and meta-analysis. BMJ. 2009. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Connock, M.; Barton, P.; Fry-Smith, A.; Aveyard, P.; Moore, D. “Cut down to quit” with nicotine replacement therapies in smoking cessation: A systematic review of effectiveness and economic analysis. Health Technol. Assess. 2008, 12, iii–iv, ix–xi, 1–135. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Lancaster, T. Interventions to reduce harm from continued tobacco use. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- Asfar, T.; Ebbert, J.O.; Klesges, R.C.; Relyea, G.E. Do smoking reduction interventions promote cessation in smokers not ready to quit? Addict. Behav. 2011, 7, 764–768. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al.; Cochrane Bias Methods Group; Cochrane Statistical Methods Group The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 (updated March 2011). Available online: http://www.cochrane-handbook.org (accessed on 21 August 2015).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Biasin meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Bolliger, C.T.; Zellweger, J.P.; Danielsson, T.; van Biljon, X.; Robidou, A.; Westin, A.; Perruchoud, A.P.; Säwe, U. Smoking reduction with oral nicotine inhalers: Double blind, randomised clinical trial of efficacy and safety. BMJ 2000, 321, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Batra, A.; Klingler, K.; Landfeldt, B.; Friederich, H.M.; Westin, A.; Danielsson, T. Smoking reduction treatment with 4-mg nicotine gum: A double-blind, randomized, placebo-controlled study. Clin. Pharmacol. Ther. 2005, 78, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.J.; Hughes, J.R.; Keely, J.P. Effect of smoking reduction on later cessation: A pilot experimental study. Nicotine Tob. Res. 2003, 5, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.J.; Hughes, J.R.; Solomon, L.J.; Callas, P.W. Both smoking reduction with nicotine replacement therapy and motivational advice increase future cessation among smokers unmotivated to quit. J. Consult. Clin. Psychol. 2004, 72, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.; Leung, D.Y.; Abdullah, A.S.; Wong, V.T.; Hedley, A.J.; Lam, T.H. A randomized controlled trial of a smoking reduction plus nicotine replacement therapy intervention for smokers not willing to quit smoking. Addiction 2011, 106, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F.; Laszlo, E.; Zellweger, J.P.; Perrot, C.; Perneger, T.V. Nicotine replacement to reduce cigarette consumption in smokers who are unwilling to quit: A randomized trial. J. Clin. Psychopharmacol. 2002, 22, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F.; Laszlo, E. Postintervention effect of nicotine replacement therapy for smoking reduction: A randomized trial with a 5-year follow-up. J. Clin. Psychopharmacol. 2007, 27, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Ebbert, J.O.; Hughes, J.R.; West, R.J.; Rennard, S.I.; Russ, C.; McRae, T.D.; Treadow, J.; Yu, C.R.; Dutro, M.P.; Park, P.W.; et al. Effect of varenicline on smoking cessation through smoking reduction: A randomized clinical trial. JAMA 2015, 313, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Gaglio, B.; Estabrooks, P.A.; Marcus, A.C.; Ritzwoller, D.P.; Smith, T.L.; Levinson, A.H.; Sukhanova, A.; O’Donnell, C.; Ferro, E.F.; et al. Long-term results of a smoking reduction program. Med. Care 2009, 47, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Hatsukami, D.K.; Rennard, S.; Patel, M.K.; Ktlyar, M.; Malcolm, R.; Nides, M.A.; Dozier, G.; Bars, M.P.; Jamerson, B.D. Efmn fects of sustained-release bupropion among persons interested in reducing but not quitting smoking. Amer. J. Med. 2004, 116, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.R.; Rennard, S.I.; Fingar, J.R.; Talbot, S.K.; Callas, P.W.; Fagerstrom, K.O. Efficacy of varenicline to prompt quit attempts in smokers not currently trying to quit: A randomized placebo-controlled trial. Nicotine Tob. Res. 2011, 13, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.M.; Hecht, S.S.; Murphy, S.E.; Lando, H.; Carmella, S.G.; Gross, M.; Bliss, R.; Le, C.T.; Hatsukami, D.K. Smoking reduction fails to improve clinical and biological markers of cardiac disease: A randomized controlled trial. Nicotine Tob. Res. 2008, 10, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Rennard, S.I.; Glover, E.D.; Leischow, S.; Daughton, D.M.; Glover, P.N.; Muramoto, M.; Franzon, M.; Danielsson, T.; Landfeldt, B.; Westin, A.; et al. Efficacy of the nicotine inhaler in smoking reduction: A double-blind, randomized trial. Nicotine Tob. Res. 2006, 8, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Wennike, P.; Danielsson, T.; Landfeldt, B.; Westin, A.; Tønnesen, P. Smoking reduction promotes smoking cessation: Results from a double blind, randomized, placebo-controlled trial of nicotine gum with 2-year follow-up. Addiction 2003, 98, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.J.; Thorlund, K.; Eapen, S.; Wu, P.; Prochaska, J.J. Cardiovascular events associated with smoking cessation pharmacotherapies: A network meta-analysis. Circulation 2014, 129, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Loke, Y.K.; Spangler, J.G.; Furberg, C.D. Risk of serious adverse cardiovascular events associated with varenicline: A systematic review and meta-analysis. CMAJ 2011, 183, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Mathew, T.P.; Herity, N.A. Acute myocardial infarction soon after nicotine replacement therapy. QJM 2001, 94, 503–504. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.; Fraser, T.; Howe, C.; Laugesen, M.; Truman, P; Parag, V.; Glover, M.; Bullen, C. Abrupt nicotine reduction as an end game policy: A randomised trial. Tob. Control 2014. [Google Scholar] [CrossRef] [PubMed]
- Burris, J.L.; Carpenter, M.J.; Wahlquist, A.E.; Cummings, K.M.; Gray, K.M. Brief, instructional smokeless tobacco use among cigarette smokers who do not intend to quit: A pilot randomized clinical trial. Nicotine Tob. Res. 2014, 16, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, M.J.; Gray, K.M. A pilot randomized study of smokeless tobacco use among smokers not interested in quitting: Changes in smoking behavior and readiness to quit. Nicotine Tob. Res. 2010, 12, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Velicer, W.F.; di Clemente, C.C.; Fava, J. Measuring processes of change: Applications to the cessation of smoking. J. Consult. Clin. Psychol. 1988, 56, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Goldstein, M.G. Process of smoking cessation. Implications for clinicians. Clin. Chest Med. 1991, 12, 727–735. [Google Scholar] [PubMed]
- Mottillo, S.; Filion, K.B.; Bélisle, P.; Joseph, L.; Gervais, A.; O’Loughlin, J.; Paradis, G.; Pihl, R.; Pilote, L.; Rinfret, S.; et al. Behavioural interventions for smoking cessation: A meta-analysis of randomized controlled trials. Eur. Heart J. 2009, 30, 718–730. [Google Scholar] [CrossRef] [PubMed]
- Lindson-Hawley, N.; Aveyard, P.; Hughes, J.R.; Lindson-Hawley, N.; Aveyard, P.; Hughes, J.R. Reduction vs. abrupt cessation in smokers who want to quit. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Lancaster, T.; Stead, L.F. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, L.; Sun, S.; He, Y.; Zeng, J. Effect of Smoking Reduction Therapy on Smoking Cessation for Smokers without an Intention to Quit: An Updated Systematic Review and Meta-Analysis of Randomized Controlled. Int. J. Environ. Res. Public Health 2015, 12, 10235-10253. https://doi.org/10.3390/ijerph120910235
Wu L, Sun S, He Y, Zeng J. Effect of Smoking Reduction Therapy on Smoking Cessation for Smokers without an Intention to Quit: An Updated Systematic Review and Meta-Analysis of Randomized Controlled. International Journal of Environmental Research and Public Health. 2015; 12(9):10235-10253. https://doi.org/10.3390/ijerph120910235
Chicago/Turabian StyleWu, Lei, Samio Sun, Yao He, and Jing Zeng. 2015. "Effect of Smoking Reduction Therapy on Smoking Cessation for Smokers without an Intention to Quit: An Updated Systematic Review and Meta-Analysis of Randomized Controlled" International Journal of Environmental Research and Public Health 12, no. 9: 10235-10253. https://doi.org/10.3390/ijerph120910235