Article Text

Abstract
Background: Few dose ranging studies have investigated optimal dosing with inhaled corticosteroids in children with asthma.
Aims: To compare the efficacy and tolerability of fluticasone propionate 100 or 200 μg twice daily in children with moderate to severe asthma for one year.
Methods: One year, randomised, double blind, parallel group, multicentre study. Children aged 4–11 years (n = 528) with moderate to severe asthma who had previously received high dose inhaled corticosteroids were given fluticasone propionate 100 or 200 μg twice daily for the 52 week treatment period. Efficacy (exacerbations, lung function, and symptoms) and tolerability (adverse events and cortisol levels) were measured.
Results: There was a non-significant decreased risk of experiencing an exacerbation at any time with fluticasone propionate 200 μg twice daily compared with fluticasone propionate 100 μg twice daily. This difference reached significance among patients with more severe asthma (defined by previous inhaled corticosteroid dose >800 μg/day). Daily record card morning peak expiratory flow (PEF) in the total population improved significantly more with the higher dose of fluticasone propionate (between group difference, weeks 1–52: 11.4 l/min). Clinic visit mean PEF improved from baseline with both doses, but the response was significantly greater with the higher dose (between group difference, week 52: 17.8 l/min). Both doses were equally well tolerated and overnight urinary cortisol concentrations were unchanged or slightly increased during treatment with either dose.
Conclusion: This long term dose comparison study shows that treatment with fluticasone propionate 200 μg twice daily may offer benefits over a lower dose, particularly in children with more severe asthma.
- asthma
- fluticasone propionate
- dose-response
- FP, fluticasone propionate
- ITT, intention to treat
- PEF, peak expiratory flow
Statistics from Altmetric.com
Inhaled corticosteroids are recommended internationally for maintenance therapy in both adults and children with asthma.1 Recent studies have shown that treatment with inhaled corticosteroids reduces hospitalisation rates and asthma related mortality.2,3 Although adequate asthma control may be achieved with low doses of inhaled corticosteroids, increasing the dose of inhaled corticosteroids for individual patients who are poorly controlled is well established in clinical practice.1 However, dose-response studies with inhaled corticosteroids in adults have shown conflicting results, with some studies showing a significant dose-response4,5 and others failing to show such a relation.6,7 Two recent meta-analyses of randomised, controlled clinical studies have investigated the dose-response effect of the inhaled corticosteroid, fluticasone propionate (FP), in adults with differing conclusions.8,9 One showed a positive dose-response with all doses of FP8 and the other did not.9
In contrast to the adult population, there have been only a few dose-response studies in children.10–13 In addition, there are concerns regarding the potential clinical consequences of systemic exposure to inhaled corticosteroids in children during long term therapy.14 While it is recognised that the inhaled corticosteroid should be titrated to the lowest effective dose, the fear of side effects and the lack of a clear dose-response may result in a reluctance to optimise the dose of inhaled corticosteroids, even in children with inadequately controlled asthma.
Fluticasone propionate has been registered for paediatric use in many countries. In some countries it is licensed for use in children aged 4 years and above at doses up to 400 μg daily for the treatment of mild and persistent childhood asthma. At this dose, significant clinical improvement is obtained with limited safety concerns. Current guidelines on asthma management in children recommend the stepwise introduction of inhaled corticosteroid therapy in children whose asthma symptoms are insufficiently controlled with once daily short acting β2 agonists.15,16
We hypothesised that a dose-response to a higher dose of FP would be demonstrable in children at the severe end of the asthma spectrum. The present study was therefore designed to compare the efficacy and tolerability of two doses of FP (100 and 200 μg twice daily) in children with moderate to severe asthma who were previously treated with high dose inhaled corticosteroids (beclomethasone dipropionate ⩾800 μg/day or equivalent). The effect of treatment on the time to exacerbation was chosen as the primary variable because it is a clinically relevant outcome measure and, as with other inhaled corticosteroids, previous studies with FP have failed to consistently show a clinically relevant increase in lung function when the dose is doubled.13
METHODS
Study design and inclusion/exclusion criteria
This multicentre, randomised, double blind, parallel group study was conducted in 39 centres in five countries in accordance with the Declaration of Helsinki. The study protocol was subject to regulatory and Ethics Committee or Institutional Review Board approval at each study centre prior to commencement. Written consent was obtained from each patient’s parent/guardian and, wherever possible, from the patient.
Children aged 4–11 years with at least a six month history of asthma and a documented requirement for high dose inhaled corticosteroid therapy were eligible for entry. All patients had received budesonide, beclomethasone dipropionate, triamcinolone acetonide, or flunisolide at dosages of 800–1600 μg/day, fluticasone propionate 400–600 μg/day, or oral corticosteroids ⩽5 mg/day, for at least four weeks prior to screening. Patients were required to have had at least one exacerbation requiring oral or parenteral corticosteroids or hospitalisation within the previous 12 months; however, hospitalisation for respiratory disease during the four weeks prior to the study was a criterion for exclusion. Children receiving long acting β2 agonists were excluded from the study, as were patients with an infection of the respiratory tract, middle ear, or sinuses.
Study treatment
The study comprised a two week run-in period during which patients continued with their previous asthma medication, followed by a 52 week treatment period. The study was initially planned to be of 16 weeks duration but was extended to 52 weeks in as many centres as possible to give greater opportunity to show an effect on exacerbation rates and allow for seasonal variations. Patients were randomised, using Patient Allocation for Clinical Trials (PACT) software, to receive fluticasone propionate 100 or 200 μg twice daily, to replace their existing inhaled corticosteroid treatment. Fluticasone propionate was administered via the Diskus inhaler as two actuations of either 50 μg or 100 μg each morning and evening.
Patients were allowed to use short acting β2 agonists as required; theophylline, sodium cromoglycate, or nedocromil sodium at a constant dose regimen were also permitted.
Assessments and outcome variables
Clinic visits were scheduled at weeks 2, 4, 8, 12, 16, 28, 40, and 52 during treatment, and daily record cards were completed by the patients (with parental assistance where necessary) throughout the study. Morning and evening peak expiratory flow (PEF), use of short acting β2 agonists, and daytime and night-time asthma symptom severity scores were recorded on the daily record card. Night-time symptoms were scored from 0 (no symptoms) to 4 (symptoms so severe I did not sleep at all), and daytime symptoms from 0 (no symptoms) to 5 (symptoms so severe that I could not go to school or perform normal daily activities). PEF was measured in triplicate at each clinic visit and the highest value was recorded. The occurrence of any adverse events was also recorded at each clinic visit. All PEF measurements were made using a mini-Wright peak flow meter. An asthma exacerbation was defined as follows: a fall in morning PEF of at least 20% below baseline value (defined as the mean of the daily record card values from the week prior to randomisation) for at least two consecutive days or an increase in the use of short acting β2 agonists on at least two occasions per day for at least two consecutive days (moderate exacerbation); a course of oral corticosteroids for up to 10 days or any treatment with parenteral corticosteroids (severe exacerbation); or any hospitalisation for asthma (very severe exacerbation).
Urinary free cortisol concentrations (relative to creatinine concentrations) were determined at the end of the run-in period and after 16 and 52 weeks of treatment using overnight (12 hour) urine collection. The Chiron ACS180 radioimmunoassay was used to measure cortisol concentrations.
Examination of returned inhalers indicated the number of doses dispensed between clinic visits, allowing treatment compliance to be calculated.
Statistical analysis
The number of participants was planned according to detection of between-group differences in time to first asthma exacerbation and time to each exacerbation. Assuming that a maximum of 55% of subjects in the fluticasone propionate 100 μg twice daily group experienced at least one exacerbation by week 8 (that is, halfway through the originally planned treatment period) and that a decrease in the exacerbation rate of 15% was the smallest clinically relevant difference, 186 subjects per treatment group were required to detect this difference at the 5% significance level with approximately 80% power.17 Thus, the aim was to recruit 450 patients to ensure adequate numbers of randomised patients.
The primary population for all efficacy and safety analyses was the intention to treat (ITT) population. On analysis of the study it became apparent that the majority of children were treated with the lowest permitted dose of inhaled corticosteroid prior to the study (800 μg per day), and therefore the asthma severity in the population might be less than anticipated. In accordance with the concept of the study, a subgroup of children treated with a dose of inhaled corticosteroid above 800 μg /day was also analysed in an attempt to measure the treatment difference in patients with truly severe asthma. Key outcome efficacy and safety measures only (exacerbations, morning, evening, and clinic PEF, and cortisol concentrations) were analysed in this subgroup.
All statistical tests used the 5% level of significance, with 95% confidence intervals. The Statistical Analysis System (SAS) software package (SAS Inc., Cary, NC, USA), version 6.12, was used throughout.
Time to each exacerbation (days) was analysed using the marginal model of Wei and colleagues,18 with terms for treatment, age, sex, and country (subjects with no exacerbations were included as censored observations). A global test of treatment effect was performed (that is, averaging across exacerbations) as well as descriptive statistics for individual exacerbations (that is, time to first exacerbation, time to second, etc). Logistic regression with terms for treatment, age, sex, and country was used for analysis of proportion of subjects with at least one exacerbation, and frequency and severity of exacerbations. All clinic visit and daily record card lung function data, as well as urinary cortisol levels adjusted for creatinine, were analysed using analysis of covariance, with terms as before in addition to baseline. Cortisol levels were log transformed prior to analysis, to satisfy normality assumptions. Symptom free days/nights and relief medication free days/nights were analysed using the Wilcoxon rank sum test, adjusted for country. Where possible, interactions between treatment and age, sex, and country were assessed at the 10% level.
RESULTS
Of 564 children screened, 528 were randomised to treatment (the ITT population). Figure 1 shows the flow of patients through the study. The two treatment groups were well matched in terms of demography (table 1). The median dose of inhaled corticosteroids at baseline was 800 μg/day (range 200–1600 μg/day) in both treatment groups, which included patients given FP at half the equivalent dose to other inhaled corticosteroids. This was the minimum inhaled corticosteroid dose required by the protocol for inclusion in the study, although 14 patients receiving lower doses were included in the ITT population (five of these were receiving oral corticosteroids, and the remaining nine were included as protocol violations). The subgroup of patients with severe asthma (defined by previous inhaled corticosteroid dose greater than 800 μg/day), comprised 100 patients in the fluticasone propionate 100 μg twice daily group and 94 patients in the fluticasone propionate 200 μg twice daily group.
Patient characteristics
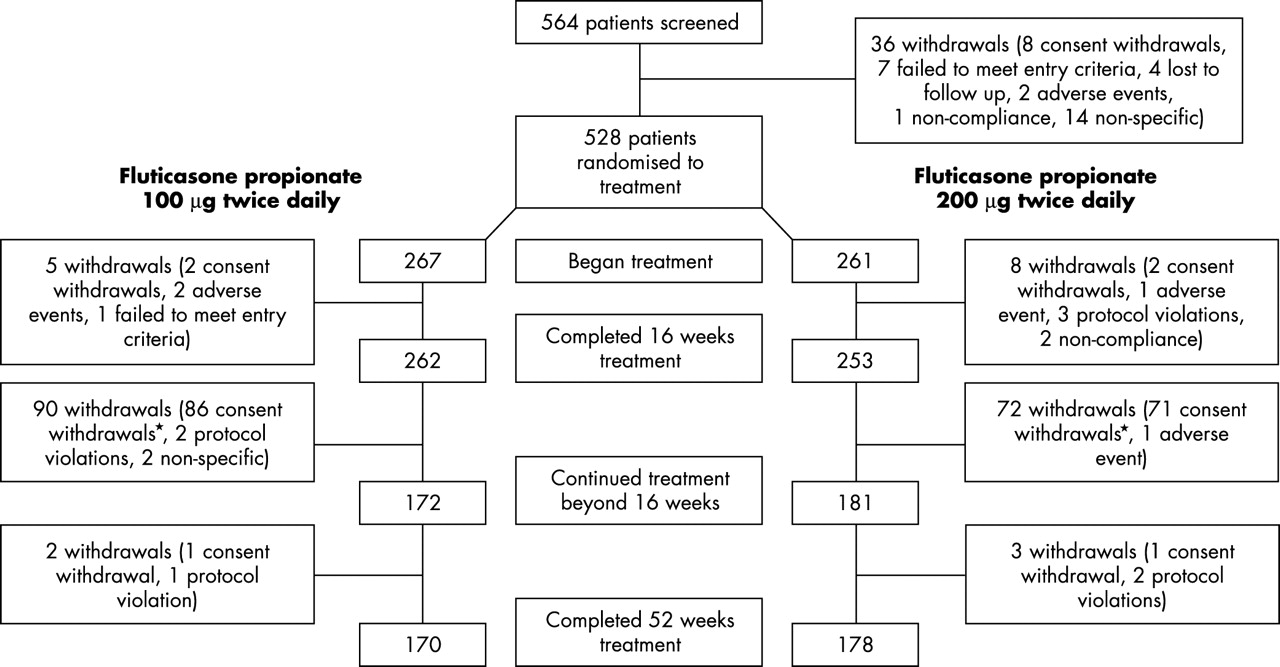
Flow of patients through the study. *Consent withdrawal: centres did not participate in the extension of the study to 52 weeks or patients did not wish to continue in the study beyond the original planned 16 weeks.
The patients were relatively symptom-free during the run-in period. During week 2 of the run-in period (baseline), the median percentage of symptom-free days was 100% in both groups. Overall, there were 64% of patients with 100% symptom-free days during week 2 of the run-in period (66% and 63% with fluticasone propionate 100 μg twice daily and fluticasone propionate 200 μg twice daily, respectively). The numbers of symptom-free nights and days without rescue medication were similarly high.
Compliance during the study was high in both treatment groups, exceeding 75% in 99% of patients. No patients withdrew from the study because of lack of efficacy.
Asthma exacerbations
The global test for a between group difference in the time to each exacerbation (irrespective of severity) in the total population, expressed as a risk ratio for fluticasone propionate 200 μg/100 μg twice daily, was 0.85 (that is, the risk of experiencing an exacerbation at any time was reduced by 15% in patients receiving the higher dose). This difference was not large enough to reach statistical significance (p = 0.182). However, with the higher dose group, for each individual exacerbation there was a reduced risk of exacerbation compared with the 100 μg twice daily dose, with the difference in risk between the groups increasing with increasing numbers of exacerbations (table 2). The subgroup analysis of patients defined as having severe asthma revealed a much larger and significant 33% reduction in the risk of experiencing an exacerbation at any time with the higher dose (risk ratio 0.67; 95% CI 0.45 to 0.98; p = 0.040). This significant result was achieved despite the reduced patient numbers in this subgroup.
Analysis of time to each exacerbation during the treatment period
Overall, the number of patients experiencing exacerbations was lower than anticipated. Only 49% and 53% of patients receiving fluticasone propionate 200 μg and 100 μg twice daily respectively reported at least one exacerbation during the 52 week treatment period (odds ratio 0.876; 95% CI 0.619 to 1.239; p = 0.454). Among the subgroup defined as having severe asthma, these proportions were 44% and 55% respectively. Of the total population, only 26 patients experienced a severe or very severe asthma exacerbation (12 in the lower dose group and eight in the higher dose group had a severe exacerbation; three in each group had a very severe exacerbation). The numbers were too small for meaningful subgroup analysis of exacerbations according to severity.
Clinic lung function
During the study, clinic PEF increased in both treatment groups. However, there was a significantly greater increase in the fluticasone propionate 200 μg twice daily group compared with the lower dose group (p < 0.05) at all timepoints (fig 2). At week 52, the adjusted mean improvement in clinic PEF from baseline was 61.7 l/min with fluticasone propionate 200 μg twice daily compared to 43.9 l/min with 100 μg twice daily (difference: 17.8 l/min; 95% CI 8.1 to 27.5 l/min; p < 0.001). The magnitude of the difference in clinic PEF at 52 weeks was similar in the subgroup of patients defined as having severe asthma compared to the entire group. However, there was a smaller number of patients involved in this subgroup (n = 55, FP 100 μg twice daily; n = 60, FP 200 μg twice daily), and this difference did not reach statistical significance (difference: 16.7 l/min; 95% CI −3.9 to 37.3 l/min; p = 0.112).

Change from baseline in mean adjusted clinic peak expiratory flow (PEF) in children randomised to fluticasone propionate 100 μg twice daily (FP 200; n = 267) or 200 μg twice daily (FP 400; n = 261). Error bars represent standard errors.
Figure 3 illustrates the extent of improvement in clinic PEF at week 52 in both treatment groups. At each specified threshold level of PEF improvement the difference between the two doses of fluticasone propionate was statistically significant (p < 0.05). A similar effect was observed in the subgroup of patients defined as having severe asthma, but again, smaller numbers of patients were involved, and the differences did not reach statistical significance.
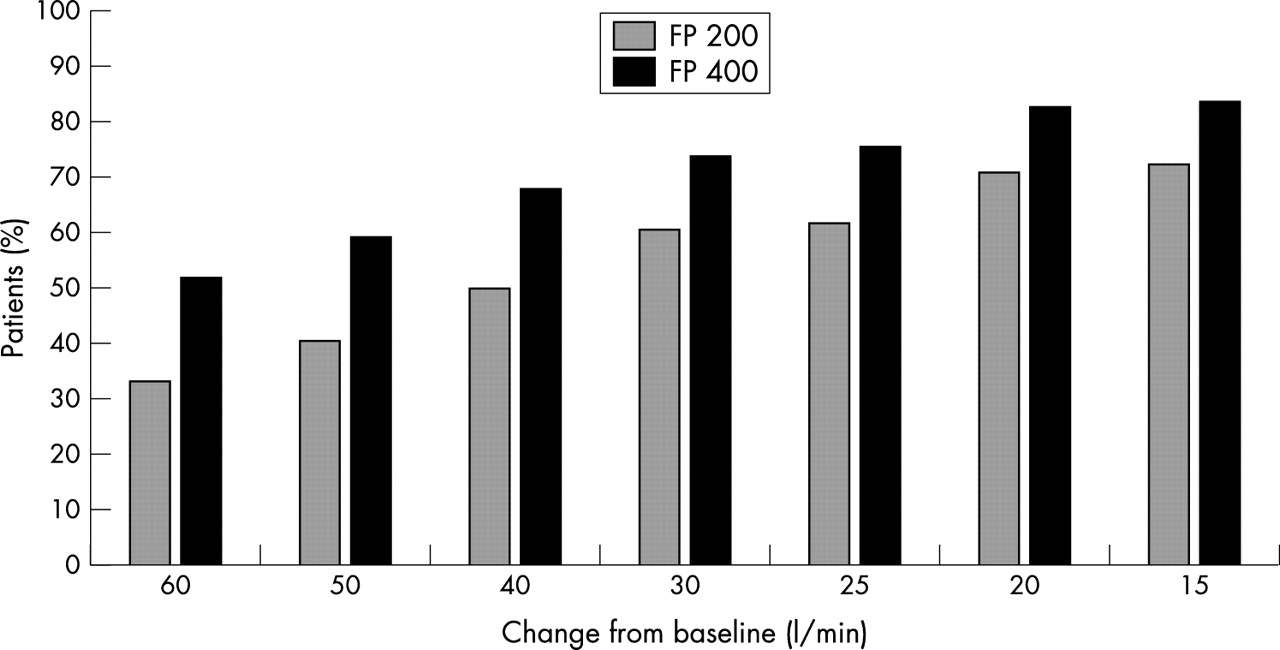
Cumulative proportion of patients showing the specified threshold change from baseline in adjusted clinic peak expiratory flow (PEF) after 52 weeks therapy with fluticasone propionate 100 μg twice daily (FP 200; n = 170) or 200 μg twice daily (FP 400; n = 178). Between group difference: p < 0.05 for each PEF threshold analysed.
Daily record card lung function
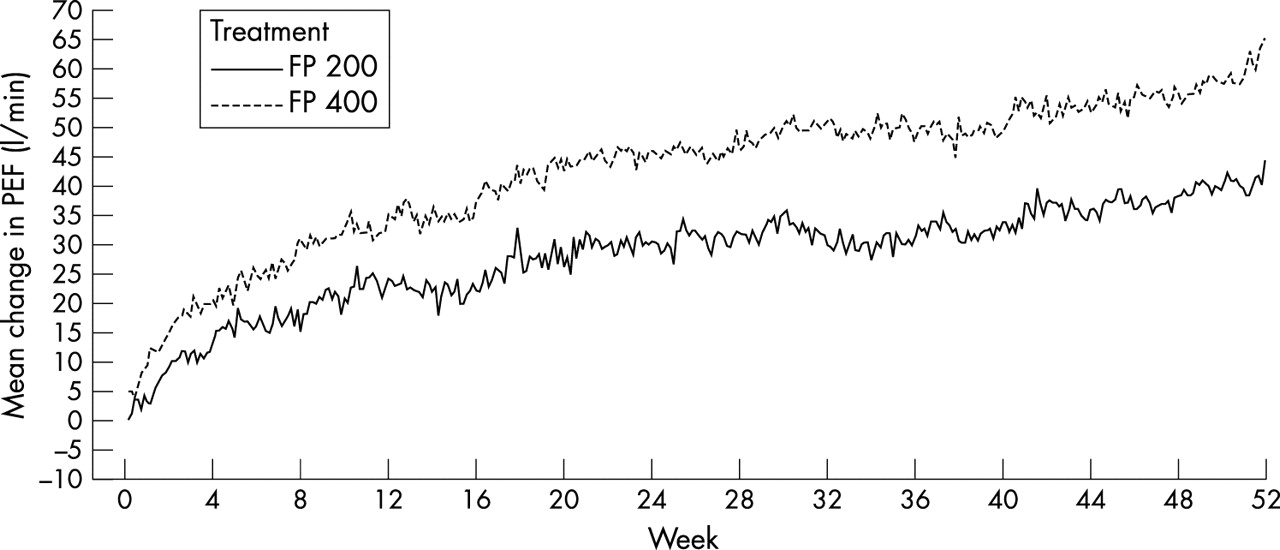
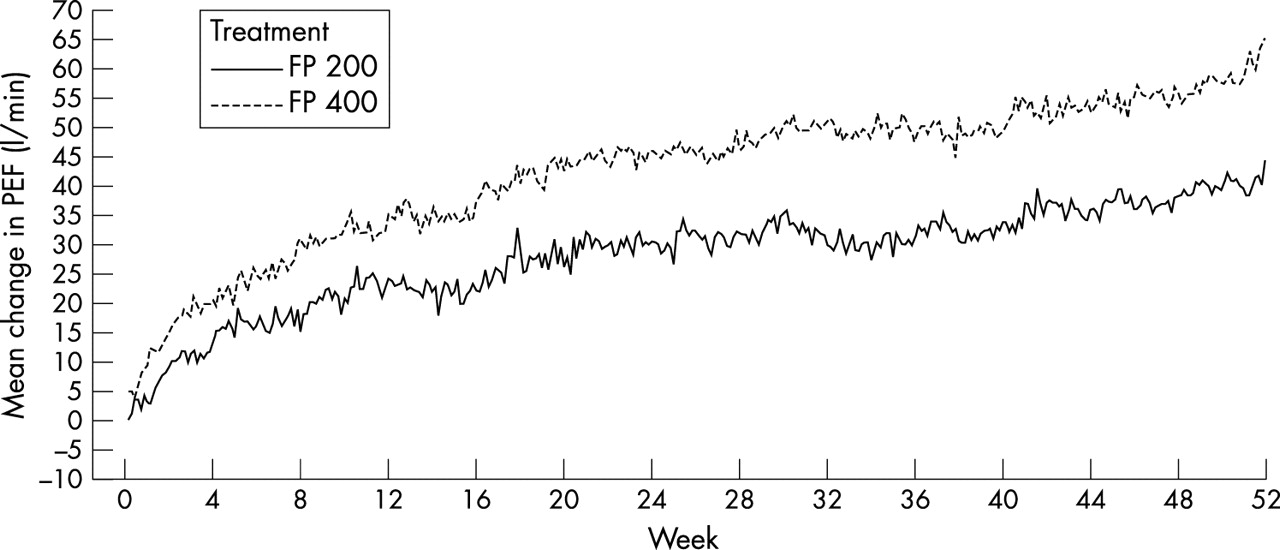
Mean morning PEF (recorded on the daily record card) increased throughout the study with both doses of fluticasone propionate, but the improvement was significantly greater with 200 μg twice daily compared with the lower dose (fig 4). Across the entire treatment period (that is, weeks 1–52), the adjusted mean changes from baseline were 33.2 l/min and 21.8 l/min in the two groups, respectively (difference: 11.4 l/min; 95% CI 5.6 to 17.3 l/min; p < 0.001). Similarly, the adjusted mean increase in evening PEF for weeks 1–52 was 30.2 l/min with fluticasone propionate 200 μg twice daily versus 18.3 l/min with 100 μg twice daily (difference: 11.9; 95% CI 6.2 to 17.6; p < 0.001). The magnitude of the difference in mean PEF was similar in the subgroup of patients defined as having severe asthma, although the statistical significance was not as strong, probably because of the smaller number of patients involved (morning PEF (weeks 1–52), difference: 10.6 l/min, 95% CI −1.0 to 22.1 l/min, p = 0.072; evening PEF (weeks 1–52), difference: 12.9 l/min, 95% CI 1.6 to 24.2 l/min, p = 0.025).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change from baseline in daily record card mean morning peak expiratory flow (PEF) in children randomised to fluticasone propionate 100 μg twice daily (FP 200; n = 267) or 200 μg twice daily (FP 400; n = 261) (unadjusted data).
Diary card symptoms
The majority of children remained symptom-free throughout the study and there were no statistically significant differences between the groups in this regard. The median percentage of symptom-free days and nights in both study groups was 98% and 97% respectively. The median proportion of days and nights with no relief medication was also similar in both treatment groups (days: 99% and 98%, for the 200 μg and 100 μg twice daily groups; nights: 99% for both groups).
Adverse events
The frequency of adverse events was similar in both treatment groups, with 58% of patients in the fluticasone propionate 200 μg twice daily group and 59% in the 100 μg twice daily group reporting one or more adverse events during the 52 week study. The three most common adverse events were rhinitis (reported by 16% and 18% of patients in the 200 and 100 μg twice daily groups respectively), viral respiratory infection (14% and 11%), and pharyngitis/throat infection (10% in both groups). There was a low frequency of drug related adverse events (6%) in both treatment groups (table 3). Most drug related adverse events were mild or moderate in severity and they resolved spontaneously; one serious adverse event (severe asthma exacerbation) was considered by the investigator to be related to study medication (fluticasone propionate 100 μg twice daily). Four patients (two in each group) were withdrawn because of adverse events attributed to study medication (chest sounds, candidiasis, anxiety, and sleeping disorders).
Number (%) of patients reporting the most common* drug related adverse events during the treatment period
Urinary cortisol
Overnight urinary free cortisol levels were unchanged or slightly increased from baseline in both treatment groups after 16 and 52 weeks treatment (table 4). The treatment ratio of concentrations (fluticasone propionate 200 μg/100 μg twice daily) was 0.86 at week 16 and 0.81 at week 52 (both p < 0.001). Similar results were seen in the subgroup of patients defined as having severe asthma.
Overnight (12 hour) urinary free cortisol concentrations, adjusted for creatinine, at weeks 16 and 52
In the total population, urinary cortisol levels remained unchanged or within the normal clinical range in 91% of children in the fluticasone propionate 200 μg twice daily group and in 95% of those receiving the lower dose. Urinary cortisol concentrations fell below the normal range (that is, <5 nmol/l) in nine patients in the fluticasone propionate 200 μg twice daily group (4%) and one patient in the 100 μg twice daily group (<1%). These changes were not considered by the investigator to be clinically relevant, and none of the patients showed clinical signs or symptoms of adrenal insufficiency. Urinary cortisol concentrations increased to levels above the normal range (that is, >40 nmol/l) in 14 patients (5%) and 13 patients (5%), respectively, in the two groups.
DISCUSSION
Fluticasone propionate 200 μg twice daily produced a decrease in the risk of asthma exacerbations compared with the 100 μg twice daily dose in children with moderate to severe asthma, which only reached statistical significance in the patients defined as having severe asthma. Both doses of fluticasone propionate improved lung function in the total population and in the subgroup defined as having severe asthma, with the higher dose being significantly more effective than the lower dose throughout the 52 week treatment period, in terms of patient recorded morning and evening PEF, and clinic PEF.
Significant differences in lung function were seen between FP 100 μg twice daily and FP 200 μg twice daily, showing a dose-response for fluticasone propionate. Previous studies have not consistently shown a dose-response in lung function when the dose of fluticasone propionate is doubled,12,13 often as a result of the near normal function in children. This was the rationale for using exacerbations as a primary endpoint in this study. However, the reduction in time to each asthma exacerbation in patients receiving the higher dose only reached statistical significance in the subgroup defined as having severe asthma. Given that many of these patients entering the study underwent a reduction in the daily microgram dose of inhaled corticosteroid therapy, it is surprising that approximately 50% of patients remained free from exacerbations throughout the 52 week study. We had expected a greater proportion of patients to experience exacerbations, particularly in the fluticasone propionate 100 μg twice daily treatment group, where the daily dose of inhaled corticosteroid was reduced by at least 50%. However, although the study was designed to recruit severe asthmatic children, the patient population was milder than desired, as suggested by the low level of symptoms and the normal (or above normal) PEF value at baseline, as well as the number of patients being free of an exacerbation. This suggests that using historical dosage of inhaled steroid may not be the most appropriate method of defining asthma severity. Inclusion of the analysis of the subset of patients that were treated with the higher dose of inhaled corticosteroid was performed to answer the original aim of the study, namely the efficacy in a severe population. The definition that we applied to categorise the patients into the severe subgroup was based on the prior dose of inhaled corticosteroid in accordance with the GINA guidelines.1 It is recommended that children >5 years with severe persistent asthma (step 4) take greater than 800 μg/day of inhaled corticosteroid (budesonide, equivalent to 400 μg/day fluticasone propionate) compared to 400–800 μg/day in children with moderate persistent asthma.
Although the inclusion criteria for participating in the study included a documented clinical requirement for the prior dose of inhaled corticosteroid, compliance with inhaled corticosteroids in clinical practice is known to be poor,19 and the improvement in PEF with both doses of fluticasone propionate may represent the improved compliance with treatment that is associated with participating in a clinical trial. While the study effect may be important, it is anticipated that this effect, if any, is similar in both limbs of this double blind trial and would not affect the treatment difference, the primary objective of the study. The inclusion of a placebo group would have been a theoretical advantage to evaluate more precisely the treatment effect, although this was not possible in the patient population we intended to recruit for ethical and safety reasons.
The lower than expected incidence of exacerbations and the improvement in PEF in this study may also be attributable to the improved therapeutic ratio of fluticasone propionate compared with other inhaled corticosteroids that has been observed in comparator studies.5,20 The patients did, however, have a high proportion of days without symptoms and without a need for relief medication at baseline. It is possible, therefore, that different asthma outcome measures are differentially sensitive to changes in the inhaled corticosteroid dosage. Indeed, a recent analysis of 19 randomised controlled trials in adults indicated that morning PEF was the most responsive and reliable outcome measure for showing a treatment effect of fluticasone propionate in asthma relative to placebo.21 The results of the present study indicate that this may also be the case for showing a dose-response relation in children.
The incidence of adverse events was similar in the two treatment groups. The small proportion of patients in each treatment group reporting drug related adverse events is similar to previous studies in children treated with similar or lower doses of fluticasone propionate.13,22–24 The low numbers of withdrawals from the present study is further evidence that fluticasone propionate was well tolerated.
Overnight urinary cortisol concentrations increased from baseline values after 16 weeks of treatment with fluticasone propionate 100 and 200 μg twice daily. After 52 weeks of treatment, overnight urinary cortisol concentrations remained raised in the fluticasone propionate 100 μg twice daily group and had returned to baseline values in the 200 μg twice daily group. The findings in the lower dose group may represent a small recovery of cortisol levels from the effects of prestudy medication. Although there were statistically significant differences in mean cortisol levels between the two treatment groups, the magnitude of the difference was small and clinically insignificant. Indeed, these differences were within the variation observed with placebo in a crossover study in healthy volunteers.25 In that study, overnight cortisol levels varied by approximately 20% between the two placebo phases. Overall, the effects of fluticasone propionate 100 and 200 μg twice daily on urinary cortisol levels in this study do not give cause for concern and were not related to any clinical sequelae. It is recognised however that urinary free cortisol concentration is a relatively insensitive marker of hypothalamic-pituitary adrenal (HPA) activity, and that a better approach would be to estimate 24 hour secretion rates of total cortisol and cortisol metabolites as derived from gas chromatography-mass spectroscopy (deemed impractical in this population)26 or a low dose Synacthen test.27 There have been a few recent case reports in children indicating that high, non-licensed doses of inhaled corticosteroids, particularly fluticasone propionate (500–2000 μg/day), can cause serious systemic side effects such as hypoglycaemia, secondary to adrenal insufficiency.28–30 It is reassuring that in the present study, using licensed doses of 100 and 200 μg/day, adrenal function tests gave reassuring results.
The increases in clinic PEF observed in this study with both doses of FP were greater than those that would have been predicted to have occurred as a result of childhood growth. For example, healthy children aged 7.8 years (the mean age of the study population) would be expected to show an annual increase in PEF of approximately 27 l/min (assuming an annual growth rate of 5 cm/year from the mean baseline height in the study population of 130 cm).31,32
In conclusion, this study showed that fluticasone propionate 200 μg twice daily produced a non-significant decrease in the risk of asthma exacerbations in children with moderate to severe asthma compared with 100 μg twice daily, the difference reaching statistical significance in the patients defined as having severe asthma. Both doses were effective in improving lung function in the total population, and there were significant between group differences in favour of the higher dose. Both treatments were equally well tolerated. Thus, this long term dose comparison study shows that treatment with fluticasone propionate 200 μg twice daily may offer benefits over a lower dose, particularly in children with more severe or uncontrolled asthma. However, in accordance with current guidelines, once control is achieved an attempt should be made to reduce the dose to the minimum that is effective without altering the control of asthma to ensure an optimal risk:benefit ratio.
Acknowledgments
This study was sponsored by GlaxoSmithKline Research and Development (FAS30006). The authors wish to thank the following investigators for their contributions to the study: M Guizova, V Ilieva, M Klinkanova, N Markova-Krouchkova, RT Racheva, P Tchakarova (Bulgaria); J Cepin-Bogovic, I Ivkovic-Jurekovic, R Lokar-Kolbas (Croatia); M Adonyi, L Barkai, I Bittera, M Farkas, K Gyurkovits, L Kosa, B Nagy, Z Novak (Hungary); J Alkiewicz, A Boznanski, D Chmielewska-Szewczyk, K Karczewska, R Kurzawa, T Latos, T Malaczynska, J Milanowski (Poland); II Balabolkin, BM Blokhin, NI Ilyina, AV Kharchev, MA Kirilov, IV Makarova, E Pashanov, LV Pushko, IB Resnik, II Sidorenko (Russia).