Article Text

Abstract
OBJECTIVE To determine the incidence and risk factors for leptomeningeal metastasis after surgery for brain metastasis of solid tumors.
METHODS Review of the records of all patients operated on for brain metastasis between January 1990 and August 1995.
RESULTS In this period 28 patients underwent surgery for brain metastasis, of whom 27 were available for evaluation in this study. Median survival after craniotomy was 11 months. Nine patients (33%) developed leptomeningeal metastasis 2–13 months after surgery, which included six of the nine patients operated on for posterior fossa metastasis (p=0.05). In five patients, leptomeningeal metastasis was the only site of recurrence. Three patients developed the leptomeningeal metastasis as bulky tumour along the spinal cord, which is a rare presentation. No other risk factors for the development of leptomeningeal metastasis other than surgery for posterior fossa metastasis were identified.
CONCLUSIONS There is an increased risk of leptomeningeal metastasis after surgery for posterior fossa metastasis. Future trials should consider the value of an active approach to this complication in these patients.
- brain metastasis
- leptomeningeal metastasis
- surgery
Statistics from Altmetric.com
Randomised studies on patients with single brain metastasis with absent or controlled extracranial tumour activity have shown a longer survival after resection followed by radiation therapy compared with radiation therapy alone.1 In his monograph, Posner mentions the development of leptomeningeal metastasis as one of the unresolved questions in surgical therapy for brain metastasis.2 In one study 38% of patients developed leptomeningeal metastasis after surgery for a cerebellar metastasis, but only 4.7% of patients treated for a supratentorial metastasis.3 An increased incidence of spinal intradural metastasis after surgery for posterior fossa metastasis was also briefly mentioned in an older publication.4 By contrast, another series with a larger proportion of patients treated for infratentorial metastasis reported only 5.5% leptomeningeal recurrences.5 However, most series on surgery for brain metastasis did not consider such recurrences. To determine the incidence of leptomeningeal metastasis after surgery for brain metastasis, we reviewed the records of all patients who had undergone brain metastasis resection in a 5.5 year period at the Daniel den Hoed Cancer Center (DHCC) in Rotterdam.
Patients and methods
METHODS
The records of all patients with brain metastasis from solid tumours treated at the DHCC in the period January 1990 to August 1995 were reviewed. Evaluable for this study were patients treated at the DHCC at the time of resection or radiation therapy of brain metastasis. Patients referred to the DHCC at a later stage of their disease (for example, for leptomeningeal disease) were excluded. We recorded the primary tumour histology, location of brain metastasis (supratentorialv infratentorial), depth of metastasis (superficial<1cm; deep⩾cm), extent of resection, postoperative therapy, diagnosis of leptomeningeal metastasis, and interval between resection and diagnosis of leptomeningeal metastasis. The extent of resection was based on the peroperative judgement of the neurosurgeon, not on postoperative imaging. The diagnosis of leptomeningeal metastasis was made if malignant cells were present in the CSF, or in the presence of typical neuroimaging findings, such as leptomeningeal enhancement extending in cerebral sulci or spinal intradural extramedullary tumour deposits.6 The survival and leptomeningeal metastasis free survival were calculated from the date of surgery to the time of study (October 1996) or to the date of death, using Kaplan-Meier survival analysis. The effect of clinical variables on survival and leptomeningeal metastasis free survival was assessed by the log rank test. The level of statistical significance was taken as p⩽05 (two sided).
PATIENTS
Twenty eight patients were treated with surgery for brain metastasis between January 1990 and August 1995. One patient, who died from cardiopulmonary failure 10 days after surgery, was excluded from further analysis. The clinical characteristics of the remaining 27 patients are shown in the table. Four patients had some evidence of progressive systemic disease at the time of surgery, which was considered of minor clinical importance. No patient was suspected of having leptomeningeal metastasis at physical examination or neuroimaging at the time of surgery. Brain metastasis was located supratentorially in 18 patients, nine patients were operated on for infratentorial lesions. Twenty five patients received adjuvant whole brain radiotherapy. Several radiation fraction schedules were used, 19 patients received an additional boost to the tumour. Two patients were not irradiated. One patient with small cell lung cancer received systemic chemotherapy. The other patient was operated on for a local recurrence of a solitary brain metastasis 6 months after radiation therapy.
Clinical characteristics of 27 patients with resection of brain metastasis
Results
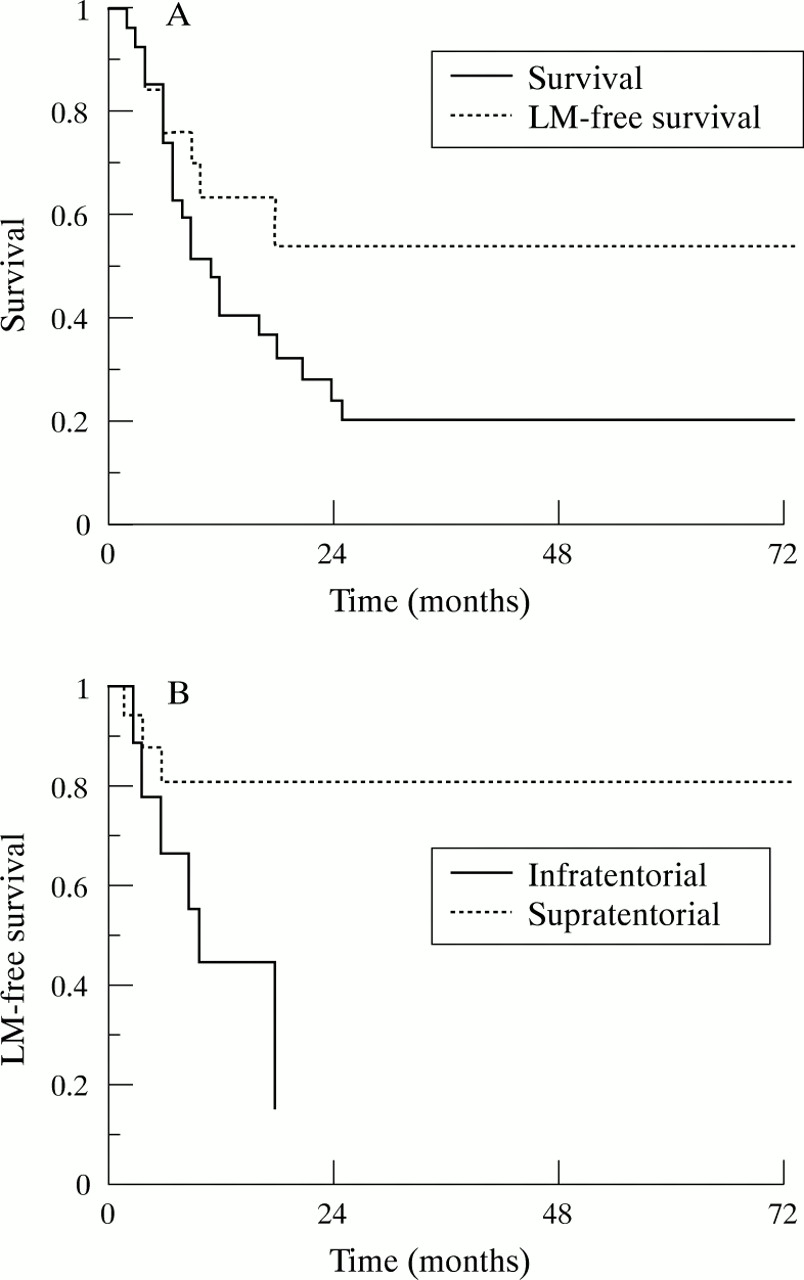
Follow up was complete in all patients. Median survival after resection of brain metastasis was 11 months (range 2 to 73 months), six patients were still alive at the time of final analysis. Nine of the 27 patients (33.3%) developed leptomeningeal metastasis. The 2 year leptomeningeal metastasis free survival was 54% (95% CI 27%–75%, fig 1). In five patients, the leptomeningeal metastasis was cytologically confirmed. In the other four patients the MRI showed typical abnormalities of leptomeningeal metastasis. In three of the nine patients with leptomeningeal metastasis MRI showed bulky intradural extramedullary tumour at the level of the cervical or thoracic spinal cord (fig 2).
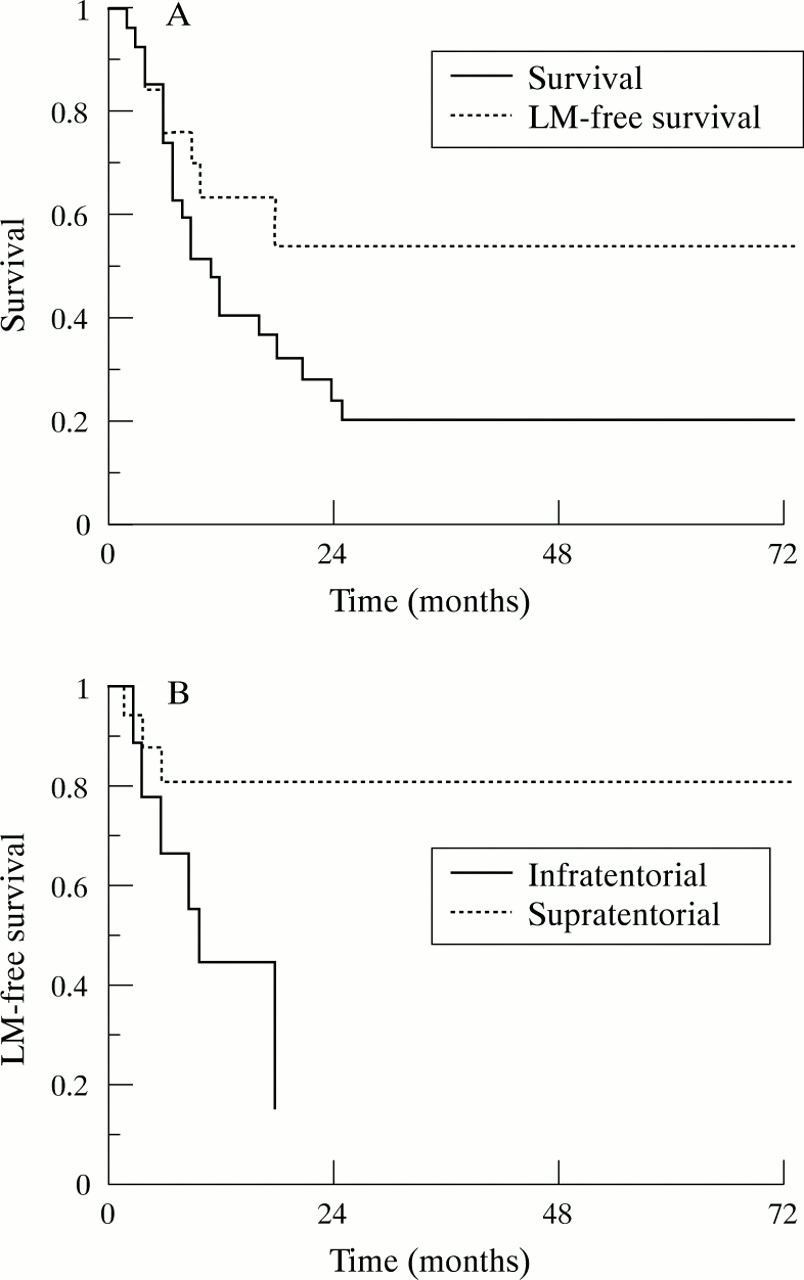
Survival, leptomeningeal metastasis free survival in the whole group, and leptomeningeal metastasis free survival after surgery for infratentorial and supratentorial brain metastasis.

{kind=link}
{kind=link}
Gadolinium enhanced MRI of the spine, showing bulky intradural, extramedulary metastasis at the level of the 5th and 6th thoracic vertebral bodies (arrow).
Nine patients had an infratentorial location of metastasis, six of these developed leptomeningeal metastasis. Three of the 18 patients (16,7%) with a supratentorial metastasis were diagnosed with leptomeningeal metastasis. The leptomeningeal metastasis free survival was significantly shorter in patients with an infratentorial lesion (fig 1, p=0.05, log rank). The extent of resection of brain metastasis, the extent of systemic disease, or treatment with an additional radiation boost were not related to development of leptomeningeal metastasis.
In five patients the leptomeningeal metastasis was the only site of recurrence of metastatic cancer after surgical removal of the brain metastasis. The other four patients had concurrent systemic or cerebral tumour recurrence (local or distant), either before or at the same time as the diagnosis of leptomeningeal metastasis. Median survival after diagnosis of leptomeningeal metastasis was 5 months (range 1 to 58 months). At the time of this study two patients with leptomeningeal metastasis were still alive, 5 and 58 months after diagnosis.
Discussion
Leptomeningeal metastasis is a relatively infrequent complication of solid tumours. The most common solid tumours associated with it are breast cancer, melanoma, and small cell lung cancer.7 8Most patients with leptomeningeal metastasis have advanced disease, only rarely is it the initial or sole presentation of cancer. In this group of 27 patients treated with surgery for brain metastasis nine patients (33%) developed leptomeningeal metastasis, in five of them this was the only site of relapse. The risk of leptomeningeal metastasis was significantly higher in patients operated on for an infratentorial metastasis. Although in four patients the leptomeningeal metastasis was not cytologically proved, we do not doubt the diagnosis as the MRI showed typical abnormalities using the criteria proposed by Freilich et al.6 Despite the high frequency of leptomeningeal metastasis, the median survival of 11 months after surgery in this group is comparable with other series on surgery for a single brain metastasis.1 3 5
The incidence of leptomeningeal metastasis in this study population exceeds that reported in studies on leptomeningeal metastasis in a cancer population. The crucial question is whether our findings should be regarded as a consequence of surgery or that they can be explained otherwise. With longer survival after surgery for solitary brain metastasis, patients are longer at risk of developing a leptomeningeal recurrence, but our data exceed the 3 year actuarial risk of 25% for leptomeningeal metastasis as found in small cell lung cancer.9 Tumours that metastasise to the brain also predispose for leptomeningeal metastasis, and the frequency is increased in posterior fossa metastasis. However, the incidence of leptomeningeal metastasis after surgery for posterior fossa brain metastasis which we found exceeds the reported 25% 1 year actuarial risk for spinal intradural seeding in fossa posterior metastasis.10 Another explanation for our findings is that leptomeningeal metastasis already existed at the time of surgery, or alternatively, that the fossa posterior tumours were in fact leptomeningeal metastasis. However, none of the patients had clinical signs or symptoms of leptomeningeal metastasis at the time of surgery.
On the other hand, intraoperative tumour spill is a well recognised complication of surgical oncology, and this may of course also happen during surgery for brain metastasis.11 Our series offers two more arguments for a relation with the surgical intervention. Firstly, leptomeningeal metastasis was a solitary recurrence in five of nine patients, whereas most patients with leptomeningeal metastasis develop this while having widely metastasised cancer. Secondly, in three of our patients MRI of the spine showed bulky intradural extramedullary tumour at the level of cervical or thoracic spinal cord (fig 2). In our experience, this is an uncommon presentation of leptomeningeal metastasis. A similar presentation of leptomeningeal metastasis after brain metastasis surgery was described by Norriset al.12 We think that these intradural metastases were due to drop metastasis, arrested along the spinal cord.
Our results are in agreement with two other studies, in which a 33%–38% incidence of leptomeningeal metastasis after removal of posterior fossa brain metastasis was reported.3 4Recently, another series reported leptomeningeal metastasis in four out of 10 patients operated on for infratentorial metastasis, by contrast with only one of 55 patients operated on for supratentorial metastasis.12 The increased risk of leptomeningeal metastasis after surgery for posterior fossa metastasis may be due to the more intimate contact with the subarachnoid space and the cisterna magna, which may offer a nidus for tumour cells not present over the cerebral hemisphere.3
These data support a postoperative screening for leptomeningeal metastasis after surgery for fossa posterior metastasis. If tumour cells are present, further treatment may be considered (either intrathecal chemotherapy in chemotherapy sensitive tumours, or neuraxis radiation in tumours resistant to chemotherapy). Future trials are needed to show whether this would be useful and to define the role of these measures.