Article Text

Abstract
Background The natural history of ulcerative colitis requires continuous monitoring of medical treatment via frequent outpatient visits. The European health authorities' focus on e-health is increasing. Lack of easy access to inflammatory bowel disease (IBD) clinics, patients' education and understanding of the importance of early treatment at relapse is leading to poor compliance. To overcome these limitations a randomised control trial ‘Constant-care’ was undertaken in Denmark and Ireland.
Methods 333 patients with mild/moderate ulcerative colitis and 5-aminosalicylate acid treatment were randomised to either a web-group receiving disease specific education and self-treatment via http://www.constant-care.dk or a control group continuing the usual care for 12 months. A historical control group was included to test the comparability with the control group. We investigated: feasibility of the approach, its influence on patients' compliance, knowledge, quality of life (QoL), disease outcomes, safety and health care costs.
Results 88% of the web patients preferred using the new approach. Adherence to 4 weeks of acute treatment was increased by 31% in Denmark and 44% in Ireland compared to the control groups. In Denmark IBD knowledge and QoL were significantly improved in web patients. Median relapse duration was 18 days (95% CI 10 to 21) in the web versus 77 days (95% CI 46 to 108) in the control group. The number of acute and routine visits to the outpatient clinic was lower in the web than in the control group, resulting in a saving of 189 euro/patient/year. No difference in the relapse frequency, hospitalisation, surgery or adverse events was observed. The historical control group was comparable with the control group.
Conclusion The new web-guided approach on http://www.constant-care.dk is feasible, safe and cost effective. It empowers patients with ulcerative colitis without increasing their morbidity and depression. It has yet to be shown whether this strategy can change the natural disease course of ulcerative colitis in the long term.
- Web-guided therapy
- ulcerative colitis
- compliance
- self-management
- cost
- 5-Aminosalicylic acid (5-ASA)
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Poor compliance with 5-aminosalicylic acid (5-ASA) treatment in ulcerative colitis due to lack of easy access to specialised inflammatory bowel disease (IBD) clinics, lack of patient education and understanding of the importance of early treatment at relapse.
Web-based concept in therapy of other chronic diseases improves the disease course, optimise patients' self-adherence, compliance, QoL and generates economic benefits for the healthcare system.
The European Council and National Health Insurance in North America have focused on empowering patients and minimising healthcare costs using new technology.
What are the new findings?
The new web-guided approach on http://www.constant-care.dk is feasible, safe and cost-effective for patients with ulcerative colitis.
The concept increases patients' compliance, quality of life (QoL), and empowerment to self-initiated treatment, and it reduces healthcare costs.
The web-based treatment strategy significantly decreased the duration of relapse.
How might it impact on clinical practice in the foreseeable future?
The new web-guided approach ‘Constant-care’ is in accordance with an action plan for a European e-Health Area, which gives patients important opportunities for improved access to better and more efficient healthcare.
Widespread implementation of the ‘Constant-care’ approach may reshape the current healthcare.
It empowers patients with ulcerative colitis in disease self-management, reduces dependency on doctors and it might possibly change the natural disease course in the long term.
The ‘Constant-care’ approach can be accommodated and used in more severe IBD patients, in some patients after surgery (pouch) and also in patients with other chronic conditions.
Background
The natural history of ulcerative colitis is characterised by relapses and remissions.1 The majority of patients with ulcerative colitis (91%) have a mild-to-moderate disease course eligible for 5-aminosalicylate acid (5-ASA) treatment.2 To prevent relapses, colectomy and colonic cancer there is a need for continuous optimisation of medical treatment via frequent visits in the outpatient clinic.1 3 Lack of easy access to specialised IBD clinics, patients' education, and lack of understanding of the importance of early relapse treatment leads to poor compliance and self-adherence.3 4 These limitations were attempted to be overcome by personalised self-management training of patients with ulcerative colitis, which successfully improved disease self-management in 96% of patients without increasing morbidity.5 Furthermore, disease monitoring by home automated telemanagement seems promising.6 Europe's healthcare needs are changing with more citizens requiring long-term care for chronic conditions,7 and European Union-wide healthcare may soon be facing financial and staffing problems.8 Health authorities believe that development of telebased services will provide cost-effective solutions. Telemedicine is the provision of healthcare services through use of Information and Communication Technology (ICT). It involves secure transmission of medical data for prevention, diagnosis, treatment and follow-up of patients. Telemedicine encompasses a wide variety of services including call/online information centres for patients, remote consultation/e-visits or videoconferences between health professionals.9–11 Telemedicine in the form of web-based therapy was successfully developed for other chronic diseases such as asthma,12 insulin-dependent diabetes mellitus,13 heart diseases and anticoagulation disorders.14 15 It improved disease course, optimised patients' self-adherence, compliance, quality of life (QoL), and reduced healthcare costs.16 The aims of this randomised control trial were first to investigate whether a self-administered, web-based e-health treatment programme during 1 year was feasible for Danish and English speaking patients with ulcerative colitis on 5-ASA therapy, second to determine whether this e-health approach could improve patient compliance, knowledge, QoL, disease outcomes, and safety and third to investigate whether the e-health approach could decrease healthcare costs primarily in Denmark.
Materials and methods
Patients
Patients aged 18 to 69 years fulfilling the international diagnostic criteria for mild/moderate ulcerative colitis treated with 5-ASA from Herlev and Amager Hospitals, Copenhagen, Denmark, and Adelaide and Meath Hospital in Dublin, Ireland, were invited by letter to participate in this study. Exclusion criteria were acute phase of co-morbid conditions (rheumatoid arthritis, chronic lung disease, coronary heart disease, chronic pancreatitis), drug (narcotic) dependence or substance abuse, use of immunomodulators (azathioprine, 6-mercaptopurine, metrothrexate or anti-tumour necrosis factor (TNF) therapy), frequent treatment (>6 months/year or two treatments per year) with high dose of systemic corticosteroids to enter remission, likely requirement of inflammatory bowel disease (IBD) surgery during the study period, previous IBD surgery, pregnancy, breastfeeding, inability to read or understand the form for informed consent or use of a computer. Eligible patients, who had signed the informed consent form, were randomly allocated to the interventional (web) or to the control group by use of randomisation program http://mahmoodsaghaei.tripod.com/Softwares/randalloc.html. Each randomisation number was placed in a closed, consecutively numbered envelope by two nurses not involved in the study. At the end of the study a historical control group (HCG) was included to test the comparability with the randomised control group. In Denmark inclusion of the HCG was carried out retrospectively from Gentofte Hospital, where neither doctors nor patients were aware of the Constant-care trial. In Ireland the HCG was included prospectively at Adelaide and Meath Hospital.
Web-based program on http://www.constant-care.dk
The details of the web-program have been described previously.17 http://www.constant-care.dk is a secured program developed and provided by PM. Each patient received a unique username and password from the investigators (ME or MS) before entering the system. Web-patients could contact the web-doctor by sending an email directly from the web-program's page ‘contact doctor’, or call/send a text message to the web-doctor's cell phone. The administrator page was used only by the investigators for weekly ‘web-ward rounds’. Patient status appeared as a simple traffic light; red indicated highly active ulcerative colitis, yellow moderate active, and green quiescent disease. This status was supplemented with patient's disease activity and QoL graphs.
Procedures
Web-intervention
All web-patients and their relatives were educated in the Patient Education Center (PEC) by ME in Denmark and MS in Ireland. Educational training (ET) included:
1.5 h disease specific PowerPoint presentation covering IBD aetiology, pathology, anatomy, medical and surgical treatment, disease course, compliance, nutrition, complications of IBD, including mortality risk and colorectal cancer chemoprevention, pregnancy and breastfeeding.
1.5 h theoretical and practical training in using http://www.constant-care.dk.
During ET the investigators aimed to ensure that each patient understood the concept, could recognise a relapse and was able to start the correct treatment guided by the e-health program. Patients were instructed to contact the study investigators if they experienced the following symptoms: More than six stools/day, daily rectal bleeding, rectal bleeding occurring between relapses, fever >37.5°C, heart rate >90 per min, severe abdominal pain and/or tenderness, symptoms persisting for more than 11 days despite intensified treatment, unexplained weight loss, or if they had any questions or doubt about the study. In Denmark, IBD patients are only treated in secondary care. Routine visits were planned as usual, but the web-patients were informed that they had a possibility to cancel their appointments, if they felt secure.
After ET the web-patients were asked to log on to http://www.constant-care.dk and follow the web-program's recommendation. In case of relapse, patients were requested to log on daily and complete the disease activity score (SCCAI)18 until they entered the green zone. Patients should then log on once a week for a total of 4 weeks after the initiation of relapse. The short form of disease specific QoL (s-IBDQ)19 should be filled in at the beginning and the end of each relapse. Once remission was achieved patients had to use the program once a month until the next relapse occurred.
Acute systemic treatment with 4 g daily of 5-ASA or more was recommended by the program based on the following symptoms: ‘rectal bleeding’ and/or ‘>3 bowel movements/day’ and/or ‘nightly stools’. The treatment was recommended for a maximum of 28 days with option to extend the high-dose period with further 28 days, if remission (green zone) had not been achieved.20 However, the extent of the acute treatment always involved the investigators' evaluation. This strategy was chosen to cover eventual spread of the disease over time and to prevent complications as toxic megacolon and colectomy. When patients entered remission, the system recommended a maintenance treatment. Additional treatment with topical 5-ASA and/or prednisolone was chosen by the patient from the list of possibilities in accordance to previously maximal extent of the disease, and patient's own experience of ‘best choice of drug’ combined with guidelines from the European Crohn Colitis Organisation (ECCO).2 21
All stored information regarding the disease activity and QoL during the last 4 weeks appeared on the web-program. Patient's treatment was updated over time. Earlier saved information could be retrieved by the patient and the doctor, allowing for disease history follow-up. Patients had screening blood tests at least annually that included: haemoglobin, liver, pancreas, kidney functions and inflammation markers.
Control patients
Patients in the control group continued the conventional treatment and follow-up in the IBD out-patient clinic. This included routine appointments, and the possibility to advance appointments if patients were experiencing relapse symptoms. The need for blood tests to monitor inflammation, and the need for sigmoideo- or colonoscopy was evaluated by the attending physician. However, patients in the control group were instructed by the investigators to fill in the SCCAI and s-IBDQ in a paper form and send it to the investigators in case of relapse symptoms as described previously. They were also instructed to fill in and send the same questionnaires 7 days after having obtained remission.
Web and control patients
All randomised patients had three visits: at baseline, at 6 months and at 12 months. At each visit, patients were asked to fill in the SCCAI, s-IBDQ, Crohn Colitis Knowledge Score (CCKNOW),22 Health Survey SF-36/SF-12,23 24 Hospital Anxiety and Depression Scale (HADS),25 and Compliance Questionnaire (CQ). The Satisfaction Questionnaire (SQ) was filled in at the 12 months visit. CQ and SQ were developed at Herlev Hospital. In case of relapse patients were asked to send in stool samples for analysis of pathogenic bacteria, Clostridium difficile, ova, parasites, and faecal calprotectin (FC) and FC again 7 days after absence of relapse symptoms. Information regarding demographic data, treatment, tests results, sick days due to ulcerative colitis and visits in the outpatient clinic was recorded in the patients' case record form (CRF). At the end of the study all patients' hospital record forms were scrutinised.
Outcomes measures
Compliance questionnaire
The compliance questionnaire (CQ) included five questions: easy access to prescription, ability of relapse recognition, following the medical doctor's advice, ability to self-initiate acute treatment, and adherence to 5-ASA treatment with dichotomised answers. In Denmark patients' answers regarding 5-ASA refill were compared with results from the e-prescription pharmacy database.
Satisfaction questionnaire
The satisfaction questionnaire (SQ) included five questions for control patients and eight questions for web patients. ≥6 cm considered as a positive answer.
CCKNOW
The CCKNOW is a 30 multiple choice questionnaire divided into four items: general IBD understanding (16 questions), medication (six questions), diet (two questions), and complications of IBD (six questions), with a scoring system of one point for each correct answer.
Short-IBDQ
The Short-IBDQ includes 10 questions derived from the 32 questions IBDQ concerning QoL. It covers four items: bowel symptoms, systemic symptoms, emotional, and social functions. The total score ranges from 10 (worst health) to 70 (best health).
SF-36
The SF-36 is a generic multi-purpose health survey with 36 questions. It yields an eight-scale profile. Scoring on a scale of 0 to 100 with mean health of 50. In Dublin SF-12 was used.
HADS
The HADS incudes 14 questions: seven on anxiety (HADS-A), and seven on depression (HADS-D). The scoring scale is divided into three groups: 0–7 normal, 8–10 borderline, ≥11 anxious and/or depressed.
SCCAI
The SCCAI is a validated symptom-based index (range 0–19) based on clinical symptoms. A score of >5 is used to define a relapse.
Faecal calprotectin
Results for faecal calprotectin (FC) were blinded for both investigators and patients until the end of the trial where the FC results were compared with the SCCAI to identify eventually over treatment. A cut-off level of ≤50 mg/kg considered normal.
Data analysis
The data were analysed as intention to treat. Time from the first relapse to remission and start of acute treatment at relapse were analysed by the log-rank test and displayed by Kaplan–Meier curves. The χ2 test was used for calculating of the compliance data. Fisher's exact test and the Student t test were used to compare the two trial arms with respect to frequency and duration of disease progressions. McNemar's test was used to compare disease activity and calprotectin measurements between the groups. Fisher's exact test was performed to compare results from CCKNOW, s-IBDQ, SF-36 and HADS. Fisher's exact and Wilcoxon tests were used for comparison of patients characteristics. Simple descriptive analyses regarding validation questionnaires were performed. A p value of <0.05 was considered statistically significant. Statistical analyses were performed using SAS version 9.2 (SAS Institute) and SPSS for Windows software 15.0.
Results
In all, 485 patients with ulcerative colitis were invited to participate of which 50% never responded and further 2% denied for practical reasons. In total, 233 patients were randomised in the Danish trial; 117 to the web and 116 to the control group; where 105 and 106, respectively, attended the baseline visit, and 89 web and 97 control patients completed 12 months follow-up. Additionally, 106 patients were included in the HCG; where 104 completed 12 months follow-up (figure 1). In the Irish trial 100 patients were randomised; 52 to the web and 48 to the control group, of whom, in total, five patients had to be excluded because they exceeded the age limit. At the baseline visit 51 and 41, respectively, attended, and 40 web and 38 control patients completed 12 months follow-up (figure 2). In Denmark, the randomisation resulted in a surprisingly different sex distribution and age at inclusion between the groups. Otherwise, there was no significant difference (tables 1 and 2).

Study profile of randomisation (Denmark). AZA, azathioprine.
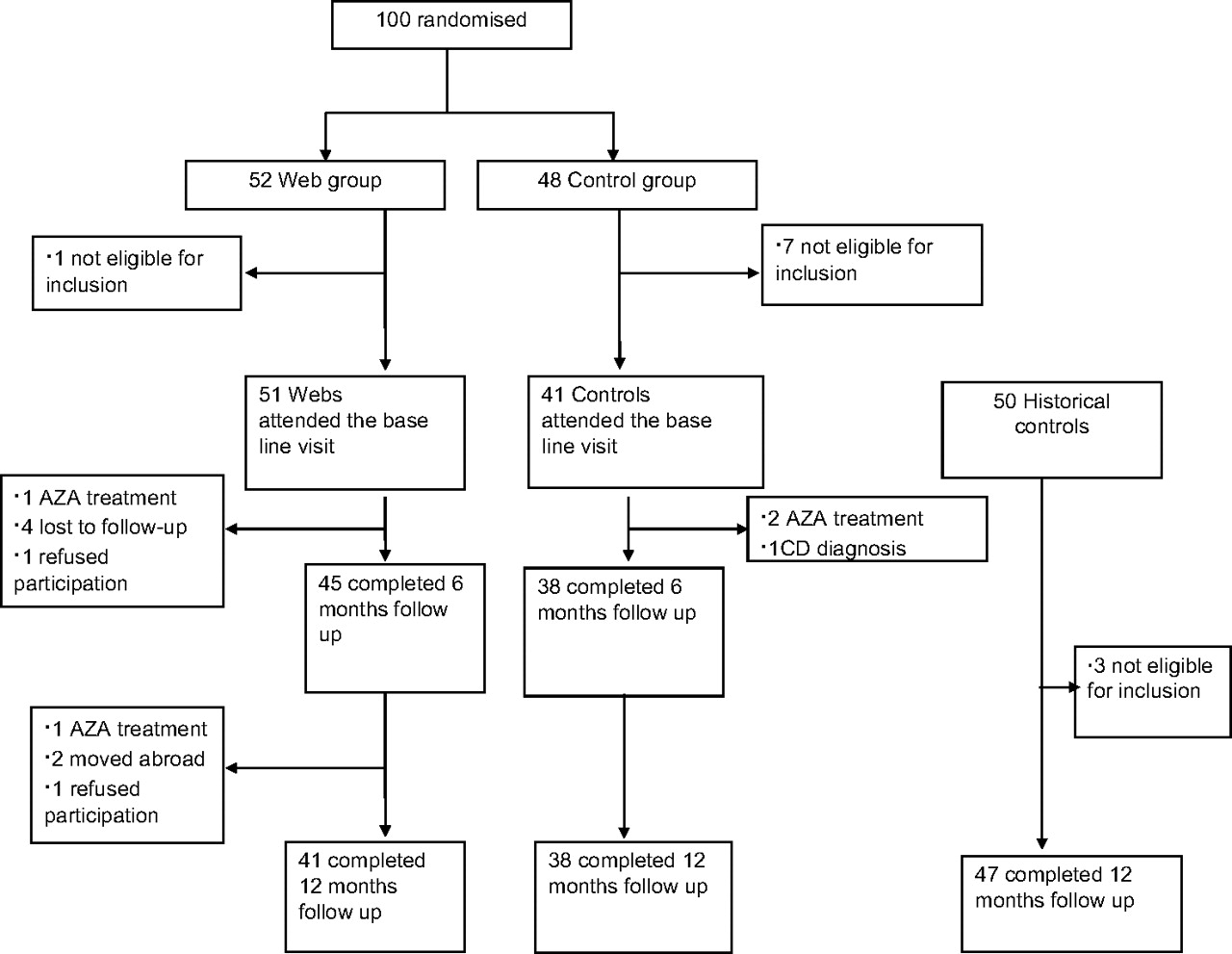
Study profile of randomisation (Ireland).
Patients description (Denmark)
Patients description (Ireland)
Denmark
Feasibility
None of the web patients were excluded due to problems with a self-initiated treatment. 88.8% found the new system feasible and wanted to continue using it; nine patients did not have a preference and one patient preferred the old system. In the control group 81.4% would like to have had the opportunity to use the new system for future management.
Compliance
At 12 months the compliance was better in web-patients than in control patients, though only adherence to 4 weeks of acute treatment was statistically significant different being 73% in the web versus 42% in control patients, p=0.005, figure 3. Community Effectiveness of the Constant-care approach (inspired by El-Seraq26 and modified to ulcerative colitis) is a multiple of the previously reported 80% remission rate on combined 5-ASA treatment20 and the patients compliance in the five compliance CQ steps presented in figure 4. Comparison of patients' actual 5-ASA treatment during the study with their refilling of medication from the e-prescription pharmacy database did not show statistical difference in patients' compliance, where 68% of web and 69% of control patients refilled at least 80% of medication.

Compliance with respect of prescription, self-recognition of relapse, following doctor's advice, self-initiating of acute treatment and adherence to 4 weeks of acute 5-ASA therapy in Denmark and Ireland.

Community effectiveness (CE) of the ‘Constant-care’ approach after 1 year in Danish and Irish patients.
IBD knowledge and QoL
At the end of the trial a significant improvement of the IBD knowledge was observed in web versus control patients (table 3).
Improvement of patients' knowledge of inflammatory bowel disease (CCKNOW) 12 months after education of the web group
Disease specific QoL was improved in the web-group, p=0.04 as well as general health, p=0.009, vitality, p=0.03, role emotional, p<0.0001 and social functioning, p=0.002 compared to control group. Depression and anxiety showed normal values in both groups; however, improvement in the depression score was observed in control patients, p=0.01.
Disease outcome
Half of the patients experienced at least one relapse during the study period, 51% in the web and 52% in the control group. Web patients reported slightly more relapses, but not statistically significant, mean 1.1 (0–6) versus 0.8 (0–4) in control group. However, relapses in the web group were of a shorter duration than in the control group (median 18 days (95% CI 10 to 21) versus 77 days (95% CI 46 to 108 days), p<0.001, figure 5. At the time of relapse 100% of web patients started treatment with high doses of systemic 5-ASA compared to 10% of control patients following the treatment regimes in the outpatient clinic, p<0.0001. Otherwise, no significant difference in use of combination of systemic and topical 5-ASA treatment was observed between the groups as well as no significant difference was found regarding number of days lost through illness, improvement of the disease activity (SCCAI ≤5), disease extension or hospitalisation. Five web versus eight control patients were treated with systemic prednisolone, and four patients (two in each arm) required hospital admission due to the need for high-dose treatment.

Time (days) from the first relapse to remission in web and control patients during 1 year of follow-up.
Faecal calprotectin
In total, 696 faecal samples were received. Forty-three samples from web-patients and 32 samples from control patients were received within 7 days of relapse. FC results were correlated with bowel frequency day and/or night and/or blood in stool. 70% of web versus 78% of control patients had FC values higher than 50 mg/kg. FC≤ 50 mg/kg observed in 50% and 57% of web versus 63% and 61% of control patients at baseline and at 12 months, respectively.
Safety
Fifteen web versus 19 control patients reported adverse events due to 5-ASA treatment. No patient died, developed toxic megacolon, or required colectomy, while three colectomies were performed in the HCG.
Cost
In total, 21 versus 107 acute visits due to ulcerative colitis symptoms and 35 versus 92 routine visits to the outpatient clinic were registered in web versus control patients, respectively, p<0.0001. Furthermore, web-patients had 24 visits related to other health problem such as prostate hypertrophy, back pain, stress, weight loss, and haemorrhoids compared to 15 visits in control group related to depression, constipation, reflux and low level of vitamin D. During 1 year, web-patients sent 86 e-mails and made 21 phone calls to the investigator versus seven e-mails and 17 phone calls made by control patients. We converted these numbers into financial saving for our department, which was 19 831 euros for 105 patients, equivalent to 189 euros/patient/year (table 4).
Economic outcome in Danish outpatient and inpatient treatment of patients with ulcerative colitis from web and control groups. The price per visit, hospitalisation and phone consultation due to the Danish Disease Related Groups (DRG) tariff per 2009 transferred to euros
The cost of actual 5-ASA medication (systemic and topical) calculated using the Defined Daily Dose During resulted in 641 euros for web versus 578 euros for control patients.
The user pattern in the HCG was comparable with that of the randomised control group, thus confirming the general clinical approach for patients treated in outpatient clinics.
Overall, we have summarised the influence of the 'Constant-Care' approach in figure 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Influence of the ‘Constant-care’ approach on the selected parameters in web and control groups after 1 year of study follow-up. 1. Feasibility of using/potential use the web-program. 2. Following medical doctors' advice at relapse. 3. Adherence to 4 weeks of acute 5-ASA treatment. 4. High dose of systemic 5-ASA at relapse. 5. Inflammatory bowel diseases. 6. Disease specific quality of life. 7. Hospital Anxiety and Depression Scale. 8. Time to remission ≤11 days at relapse. 9. Disease activity improvement (SCCAI≤5). 10. Faecal calprotectin >50 mg/kg. 11. Compliance with systemic and topical 5-ASA treatment during the study.
Ireland
88% of web patients' found the new system is feasible in English and wanted to use it in the future; four patients did not have a preference and one preferred the old system. 68% from control group would like to have the possibility to use the new system for future management.
Only adherence to 4 weeks of acute treatment was statistically significant in the web-group 73% versus 29% in control patients, p=0.03, figure 3. Community effectiveness of the Constant-care approach is shown in figure 4. There was no significant difference in improvement of IBD knowledge or disease specific QoL between the groups. However, improvement of general QoL as mental health, p=0.01, physical functioning, p=0.03 and social functioning, p=0.02 were observed in web-patients. Depression and anxiety showed normal values in both groups with anxiety improvement in web-patients, p=0.02. 39% of web and 24% of control patients reported at least one relapse during the study period. The mean of relapse frequency was 0.6 (0–4) in web versus 0.2 (0–1) in control group, p=0.02. However, relapses in the web group were of a shorter duration than in the control group (observed median 30 (2–37) versus 70 (7–217) days), p<0.03. At the time of relapse only 15% of web versus 10% of control patients started treatment with high doses of systemic 5-ASA. At the end of the trial no significant difference was observed between the two arms in number of days lost through illness, improvement of the disease activity, disease extension or hospitalisation. Three web patients versus two control patients required hospital admission due to high dose systemic prednisolone treatment. In total, 99 faecal samples were received. Twelve samples from web and one sample from controls patients were received within 7 days of relapse, which was not sufficient to compare with the relapse symptoms for over treatment calculation. FC ≤50 mg/kg was observed in 45% of web patients at baseline and 22% at 6 months visit and 45% of control patients at 6 months visit. Comparison between FC results at 12 months and baseline in control group was not possible due to small numbers of the samples. None of the patients reported adverse events. No patient died or had toxic megacolon. One control patient required colectomy after exclusion from the trial due to azathioprine treatment and histology showed Crohn's disease. In total, 62 versus 91 routine visits to the outpatient clinic were registrated in web versus control patients, respectively, p=0.007 and 9 acute visits in both groups. Furthermore, web patients had eight visits related to hidradenitis suppurativa and nutrition questions compared to four visits in control group due to anticoagulant treatment and nutrition. The HCG was comparable with the control group.
Discussion
Our study showed that the new web-based approach ‘Constant-care’ for mild/moderate ulcerative colitis patients in 5-ASA treatment was feasible in both Denmark and Ireland, two European countries with different languages. 88% of both Danish and Irish patients preferred this approach to conventional care. Patients empowered to self-initiate 5-ASA treatment by the web-guided solution felt safe with web-doctors follow-up online. At relapse, all Danish web-patients treated themselves with high doses of systemic 5-ASA compared to only 10% of control patients treated in the outpatient clinic. No difference was observed in occurrence of adverse events or hospital referred serious adverse events, ‘Constant-Care’ resulted in better adherence to 4 weeks of acute treatment in the web-group than in the control-group, the difference being 31% in Denmark and 44% in Ireland, and it gave a better community effectiveness, being 24% higher in the web-group than in the control-group in Denmark and 33% in Ireland. The patients' education, which is an important component of the web-based approach, significantly improved the Danish patients' general IBD knowledge and disease specific QoL without increasing patients' morbidity, depression and anxiety. Irish patients, however, did not show any improvement in the IBD knowledge. As expected, half of Danish patients reported at least one relapse during the 1 year follow-up. Sufficient systemic 5-ASA treatment in all relapsing web patients as recommended in ECCO guidelines21 resulted in a shorter median duration of relapse in the web-group than in the control group, the difference being 59 days. In Ireland unexpected, only 24% of control patients reported a relapse, and only 10% and 15%, respectively, of relapsing patients used sufficient systemic 5-ASA treatment. Even so, a shorter duration of relapse was observed in the web-group. In Denmark we were able to show via the FC test that no patients were over-treated, thus supporting our previous described results.27 Unfortunately, compliance with faecal samples during relapses was very low in Irish patients, which prevented us from validating possible over-treatment. An explanation could be the study design, in which patients received the FC results only at the end of the study, leading to misunderstanding of the importance of this aspect, or it could be due to a reluctance to supply a sample of stool. The Danish web-patients made 86 acute outpatient visits fewer than control patients despite reporting slightly more relapses. Web-patients were instructed to contact the study investigator in case of any doubt or questions. This resulted in more e-mails and phone calls from the web-patients. Despite this, the web-based self-management decreased treatment costs by 189 euros per patient during 1 year of follow-up. However, there is no DRG tariff for eHealth care in Denmark yet. In Ireland, the web-patients had 29 routine visits fewer than the control patients, but no difference was found in number of acute visits. With regard to the differences in outcome measures between Denmark and Ireland, variations between healthcare systems, standard treatment schemes for IBD patients in outpatients clinics and/or general practice, patients' mentality, and economic limitations have to be taken into account.
The new web-based treatment approach ‘Constant-care’ intertwines with the action plan for a European e-Health Area,10 which gives patients important opportunities for improved access to better and more efficient healthcare. Widespread implementation of this approach may reshape the current healthcare, and it could lead to savings in both time and costs. Overall, the Constant-care concept seems to empower patients with ulcerative colitis to self-management and to reduce their dependency on doctors. Furthermore, this approach can be accommodated and used in more severe IBD patients, in some patients after surgery (pouch) and also in patients with other chronic conditions.
In conclusion, the new web-guided approach on http://www.constant-care.dk was shown to be feasible, safe and cost-effective for patients with ulcerative colitis. By implementing the web-based treatment strategy, the duration of relapse decreased significantly. It has yet to be shown whether this strategy can change the natural disease course of ulcerative colitis in the long term.
Acknowledgments
We are grateful to the IBD nurses Lene Neergaard and Anna Svendsen from Herlev University Hospital for their great enthusiasm and important input to this work. We appreciate the statistical help provided by Jens-Kristian Slott Jensen. The use of the Inflammatory Bowel Disease Questionnaire authored by Dr Jan Irvine et al was made under licence from McMaster University, Hamilton, Canada.
References
Footnotes
Funding Colitis Crohn Patient Organisation, Moran's Foundation, Vibeke Binder & Povl Riis' Foundation, Bayer Health Care Funding, Augustinus Foundation, Munkholms Foundation, Tillotts Funding, Scientific Council at Herlev Hospital, Prof. Fagerhol Research Foundation, Aase & Einar Danielsen Foundation, Ole Trock-Jansen & Hustrus Foundation, and European Crohn Colitis Organisation.
Competing interests PM is member of the advisory boards in Ferring, Tillots, MSD and Swedish Orphan. ME is member of the advisory board in Swedish Orphan. HS is member of the advisory board in Swedish Orphan. CO'M is on the International Advisory Board of Abbott, MSD, and Shire Pharmaceutical Company. He has unrestricted educational grants from Abbott and MSD.
Ethics approval This study was conducted with the approval of the Danish Ethical (KA 05115) and Irish Ethical Committee of St James's Hospital and the Adelaide & Meath Hospital incorporating The National Children Hospital at Tallaght.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Digest