Article Text

Abstract
Background Motor vehicle accidents associated with commercial driving are an important cause of occupational death and impact public safety.
Objectives We summarise the evidence regarding the type, prevalence and impact of medical conditions discovered during health assessment of commercial drivers.
Evidence review We conducted a systematic review of multiple electronic databases and made a manual search for relevant studies that enrolled commercial drivers in any country and reported the outcomes of health assessment carried out in the context of commercial driving through November 2012. Data were extracted by a pair of independent reviewers and synthesised using a metanarrative approach.
Results We identified 32 studies of moderate methodological quality enrolling 151 644 commercial drivers (98% men). The prevalence of multiple health conditions was high (sleep disorders 19%, diabetes 33%, hypertension 23% and obesity 45%). Some conditions, such as sleep disorders and obesity, were linked to increased risk of crashes. Evidence on several other highly relevant medical conditions was lacking. Cost-effectiveness data were sparse.
Conclusions Several medical conditions are highly prevalent in commercial drivers and can be associated with increased risk of crashes, thus providing a rationale for health assessment of commercial drivers.
- Occupational & Industrial Medicine
- Qualitative Research
- Preventive Medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This systematic review followed a rigorous methodological approach to summarise the type, prevalence and impact of medical conditions discovered during health assessment of commercial drivers.
-
Data were insufficient to conduct quantitative analysis and provide pooled estimates.
-
The available evidence is at high risk of bias due to reporting and selection biases.
Introduction
Driving commercial motor vehicles is defined as a class of professional driving that requires a special license and qualifying skills to operate on certain types of machineries for commercial use.1 In the USA only, there is an estimated 11.4 million commercial vehicle drivers.2 Transportation accidents, particularly roadway accidents, are considered as the cause of workplace deaths, contributing to about 41% of deaths among all-cause deaths.3 In 2012, commercial driving was reported as the leading causes of occupation-related deaths among all-occupational deaths accounting for about 50% of all-work injury deaths.3 It accounts for third highest fatal occupation. Motor carriers employing commercial drivers encounter steep economic consequences from accidents resulting from impaired or incapacitated drivers.4 For example, it is estimated that each accident where the driver involved had an obstructive sleep apnoea syndrome (OSA) would approximately cost US$59 000 in direct costs and liability.5
The Federal Motor Carrier Safety Administration (FMCSA) is an agency within the US Department of Transportation (DOT) charged with regulating interstate commerce involving commercial motor vehicles. The FMCSA has published statutory regulations for commercial drivers, mandating a medical examination at least every 2 years, and more frequently for drivers with specific medical conditions that require more frequent follow-up. The medical regulations in the USA differ from other countries. Commercial driving vehicle collisions have resulted from various health-related events or condition,6 including sleep disorders (eg, OSA),7 fatigue,8 diabetes mellitus (DM),9 hypertension and the use of illicit drugs, making the commercial driving medical examination a major individual and public safety priority. OSA is a significant health problem that is estimated to affect about 20% of adults in general population10 and about 28% of commercial drivers.11 OSA can cause daytime sleepiness, fatigue and poor concentration, as well as night-time snoring and restlessness, all of which is attributed to sleep arousals and poor-quality sleep. Hypertension has also been associated with increased risk for acute life-threatening events, thereby resulting in higher crash risk.12 The prevalence of obesity among commercial drivers may also result in musculoskeletal compromise, and the association with elevated body mass index (BMI) and crashes has been documented.7 These and other medical conditions pose potential risk for the drivers and other individuals on the road while the driver is on duty.
The impact of interventions to evaluate and assess fitness-to-drive among drivers in general population with chronic conditions was studied.13 A prior systematic review concluded that certain clinical and neuropsychological tests lacked sufficient evidence in predicting fitness-to-drive end points, or the ability to reduce motor vehicle crashes in drivers with chronic disabilities.13 The evidence, however, continues to be conflicting, particularly involving commercial motor vehicle drivers. For example, the association between untreated OSA and motor vehicle collision rates is well identified,14 and well-managed OSA has been associated with decreased collision rates.15 Conditions such as hypertension, obesity, fatigue and DM have all been found in many commercial drivers involved in accidents.12 However, determining a cause–effect relationship between these medical conditions and crash cases can be challenging.
In this systematic review, we aim to appraise and summarise the existing evidence regarding the health assessment of commercial drivers including various types of examinations for fitness-to-drive. We plan to evaluate the outcomes of these assessments in terms of prevalence and type of conditions detected, the economic impact of these conditions and their association with crashes, and how they are diagnosed in commercial drivers. Such information can provide a rationale for the fitness-to-drive examination and help policymakers and clinicians conducting these examinations.
Methods
The analytical framework of this meta-narrative review is depicted in figure 1. We hypothesised that the finding of prevalent conditions in commercial drivers that can be associated with increased risk of crashes and can be readily diagnosed would provide the rationale for the fitness-to-drive examination. Possible downsides and burdens of such examination are also presented in the framework. We also aimed at searching for diagnostic tests evaluated specifically in this population since the diagnostic accuracy of tests may be different in commercial drivers than the general population (due to different disease prevalence, comorbidities, issues with under-reporting, etc). If we only find sparse evidence about conditions known to impact driving, such gap in the evidence would provide research agenda for future studies in commercial drivers.

Analytical framework.
Literature search and study eligibility
We included original observational studies, prospective and retrospective studies that enrolled commercial drivers screened to evaluate their fitness-to-drive regardless of the country of origin. Economic studies that assessed costs related to physical examinations or crash costs in commercial drivers with medical assessment history were also included. Health assessment and evaluation search terms included physical examination, visual acuity tests, drug screening, sleep pattern and fatigue syndromes assessments, health questionnaires in relation to driving risks and psychological and neurological evaluations. Studies that examined drivers through driving tests, on the road or through driving-simulation scenarios, were also included. We expanded the search to include a broad spectrum of health-related conditions studied in commercial-vehicle drivers, acute or chronic; however, OSA, hypertension, obesity, alcohol misuse, use of illicit drugs and diabetes were the most prevalent studies identified. We expanded the search to include all languages, with last date of inclusion to be November 2012.
A comprehensive literature search was conducted by an expert reference librarian with input from a study investigator with experience in systematic reviews (MHM). The search included the electronic databases MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, CINAHL and Scopus, using various combinations of controlled vocabulary supplemented with key words. We also searched FMCSA documents and website for additional references, and to examine the current non-discretionary and discretionary medical requirements. Two reviewers (AMAD and BF), working independently, identified original studies eligible for further review by screening abstracts and titles. If a study was deemed relevant, the manuscript was obtained and reviewed in full-text versions for further assessment. Previously described data sources, including citing articles and relevant systematic reviews were searched manually for possible studies, and duplicates were excluded.
Data extraction
Two reviewers independently extracted data. We extracted data on patients’ demographics, baseline characteristics, study design variables, sample size, intervention type, study medical examination focus and outcome measures when reported. In addition, for each study, we extracted variables related to the medical history or the physical examination that were used for assessment, including blood pressure (BP) measurements, BMI, neck measurements, history of chronic illness and disease-specific scores, when possible.
Risk of bias assessment
We used The Newcastle-Ottawa Scale (NOS)16 to appraise the risk of bias (methodological quality) of the included studies. For diagnostic studies, we used the QUADAS tool.17 For economic studies, we used the National Institute of Health and Care Excellence (NICE) and Consolidated Health Economic Evaluation Reporting Standards (CHEERS) guidelines.18 ,19 For cross-sectional studies, we evaluated patient selection, reference standard and inclusion of index cases, standardised follow-up and robustness of outcome ascertainment.
Data synthesis
After conducting the literature review and thoroughly observing the methodological heterogeneity between studies, and the non-standardised use of the commercial driver’s license medical examination, insufficient reporting of effect size of measurements and diversity in range of data sources, we synthesised the evidence using a meta-narrative approach according to the RAMESES guidelines20 and did not pursue meta-analysis. A meta-narrative systematic review follows the phases of planning, search, mapping, appraisal and synthesis. Synthesis phase consists of identifying the key dimensions of the problem, providing a narrative account of the contribution of each dimension, explaining conflicting findings and considering the higher order data. Data are presented using descriptive statistics and or narratively without quantitative pooling.20 For the purpose of this review, we considered the various terms used for the medical evaluation of commercial drivers interchangeable (eg, commercial driver's license physical examination, fitness-to-drive, health assessment and evaluation, etc).
Results
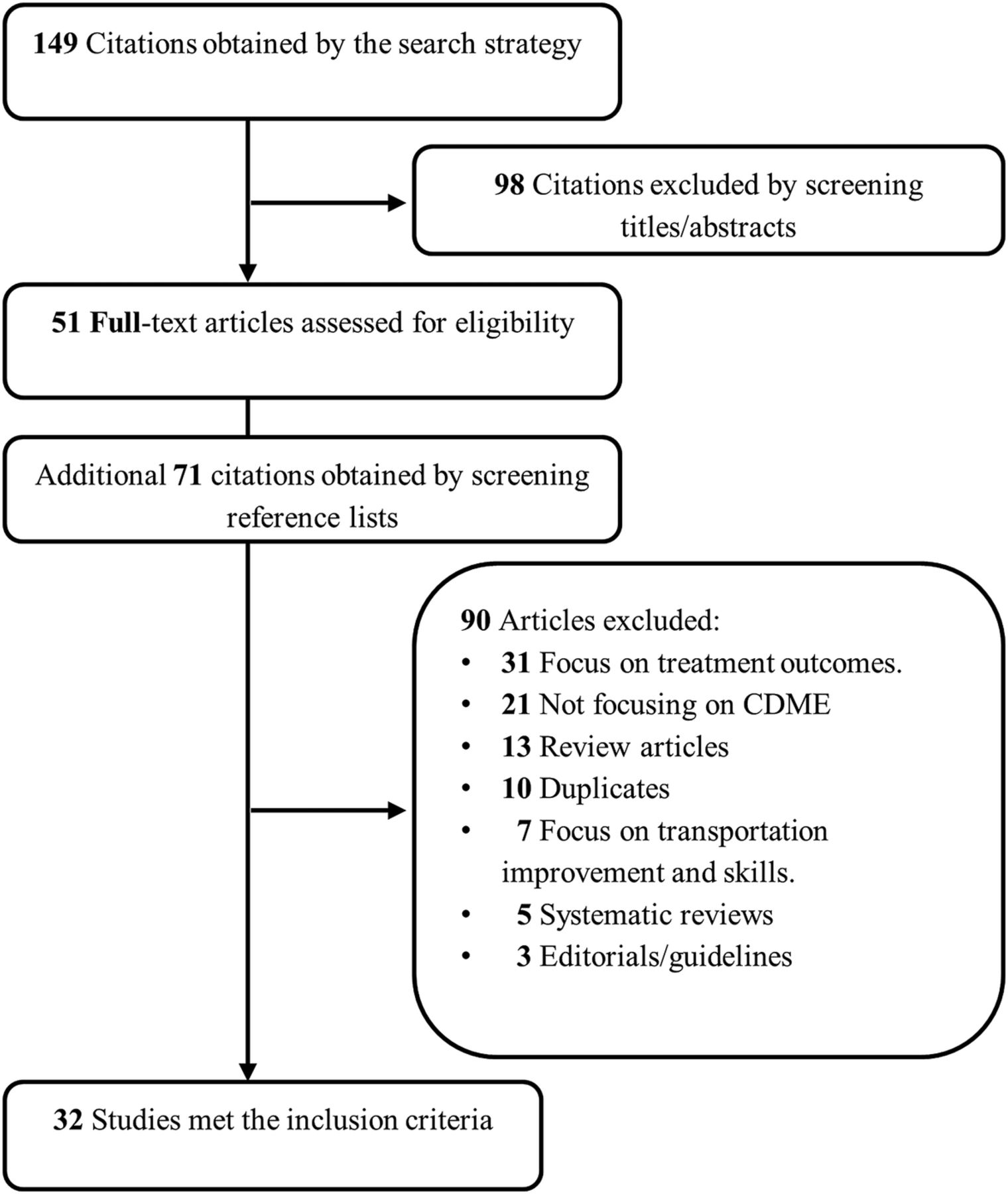
We included 32 studies (figure 2) that enrolled 151 644 drivers (age 28–63; 98% men, with a majority of Caucasian or Asian ethnicity). Table 1 summarises and describes the included studies. Online supplementary table S1 summarises the baseline characteristics of included studies.
Description of the included studies

{kind=link}
{kind=link}
Flow chart of the literature search.
The studies examined different health conditions, except for four studies, that combined more than one medical condition; 19 studies concentrated on OSA or other sleeping disorders, three studies on hypertension or BP control programmes, two on DM and four were related to studying the use of drug and alcohol consumption. There were three economic and cost-effectiveness studies in different conditions in commercial drivers. Included studies contained different designs; 16 studies were cross-sectional, 7 diagnostic studies, 4 cohort studies and 5 case–control studies. Three of the 16 cross-sectional studies were economic studies. Seventeen of 32 studies originated from the USA. Online supplementary table S2 describes the methodological quality of the included studies. The overall quality of the body of evidence was moderate to low. The main findings of included studies are summarised in table 2.
Summary of the main findings of included studies stratified by condition
Prevalence data
Sleep disorders were present in 19.2% (n=2674) of the participants. OSA constituted the main sleep disorder. DM prevalence was 33.4% (n=16 138), with a mean crash rate of 25% (table 2). The average BMI was 30.5±6 kg/m² and mean age of 47 years, with no clear distinction of diabetes type. The prevalence of hypertension was 23% (n=1000, mean age 43, BMI≥30 kg/m²). The prevalence of alcohol and/or illicit drug use was 0.3% (n=6413), compared with 5.4% of car and van drivers24 ,32 The prevalence of overweight and obesity was 78.4% and 45.2%, respectively.
We did not find studies that reported on other highly relevant medical conditions, such as seizure syndromes, hearing and visual impairments (one study on binocular vision) or chronic kidney disease.
Association with crashes
Studies generally agreed on finding an association between obesity and the risk of crashes. This was more evident in the presence of comorbidities, especially with concomitant sleep disorders and fatigue syndromes.7 A systematic review demonstrated that treatment of OSA with continuous positive airway pressure reduces the risk of crashes by 72%.15
Patients with DM were at increased risk of crashes; and6 ,25 ,38 also at increased risk of OSA and more prone to accidents when compared with those with no diabetes (16.2%; OR 2.03, CI 1.51 to 5.70).25 The use of insulin, oral hypoglycaemic agents or both showed an increased relative risk of crashes, as did low glycated haemoglobin (HbA1c) quartiles and severe hyperglycaemia requiring an outside assistance (OR=4.07, 95% CI 2.35 to 7.04).38 Bus or truck drivers with diabetes showed no significant relationship with crash severity.38
Hypertension in bus drivers and binocular vision problems in truck drivers were associated with increased crash severity.9 Surprisingly, illicit drug use was not linked to increased risk of accidents.32
Diagnostic strategies
Various sleep screening tests and questionnaires (see online supplementary table S3) including Epworth Sleepiness Scale,28 ,30 ,33 ,35 ,36 ,43 ,46 Berlin questionnaire26 ,30 ,41 and the Consensus Criteria50 were used to evaluate the presence of sleep disorders in commercial vehicle drivers, the latter showing marked sensitivity in this setting.25 ,37 ,43 Other modalities were less commonly used (polysomnography, actigraphy, analysis of cyclic variation of heart rate from automated ECG and the Multivariable Apnoea Prediction Index).22 ,23 ,27 ,34 Some studies used on-road vehicle motion data as well as video of the drivers and the surrounding environment to analyse driving or patterns while driving.7
A program that couples diagnosing hypertension with an intervention (the DownShift program) was associated with improved BP control and use of medications, high participant satisfaction and low risk of driver's disqualification.31 ,44 Various screening tests were used to evaluate illicit drugs and alcohol misuse.24 ,32 In general, there was limited evidence favouring a particular strategy in commercial drivers beyond what is known from studies in the general population.
Economic impact
Screening for OSA in commercial drivers using polysomnography was found not to be cost-effective (more expensive than the cost of crashes when no screening is carried out). However, a stratification approach using BMI, age and gender with subsequent confirmatory in-lab polysomnography for high-risk drivers was cost-effective if 74% of those diagnosed accepted treatment.51
Overweight and obese truck drivers were found to have significantly higher annual healthcare cost when compared with normal weight participants.42 These individuals had higher prevalence of hyperlipidaemia, diabetes and hypertension,42 suggesting possible cost saving if screening and management of obesity lead to reduction in the incidence of obesity complications.
In hypertension, the economic impact of the 2-year BP DownShift program showed cost savings and cost reduction when compared with the pre-BP DownShift phase to the utility company studied.40 These data are from a single study; however Zaloshnja et al45 reported the annual employer cost of motor vehicle crashes in which at least one driver was alcohol-impaired was over US$9 billion and reported significant costs related to crashes while on job, as well as for workplace violence-related injuries.
Discussion
We conducted a systematic review of the literature and demonstrated that several conditions are significantly prevalent in commercial drivers and can be associated with increased risk for crashes. There were limited data about the burden, cost and possible down sides of the fitness-to-drive examination. Health assessment of commercial drivers seems to be well justified although more studies are needed to provide evidence for the best diagnostic strategies in this population. We did not find studies about several conditions that are highly relevant to driving (eg, seizure disorders, visual impairment, substance abuse and others) likely due to under-reporting. Individuals with or at risk of these conditions are either not allowed to drive commercially or choose to not enrol in screening studies. Cost-effectiveness data are limited but seem favourable when a staged diagnostic approach is used for OSA or when screening was associated with an intervention to control hypertension.
There are several challenges that face commercial vehicle drivers and their medical examiners. Drivers tend to under-report OSA symptoms22 because of their concerns about losing their certification and also because of the lengthy and expensive subsequent tests that may not be covered by insurance or employer; and also due to loss of income during the medical evaluation. However, several studies21 ,23 ,25 ,26 ,34 ,37 ,39 ,43 tested the effectiveness of single and in-home adherence-monitored sleep disorders testing and therapy and found it to be helpful. Reporting and selection bias affected these studies as they depended on subjective reporting or enrolled drivers with more severe conditions. Varying definitions of sleep disorders are also another challenge.
Evaluating and managing commercial drivers with diabetes remains controversial. Risk of crashes can increase in those with uncontrolled diabetes and in those with tightly controlled diabetes at risk of hypoglycaemia.38 Drivers with diabetes are likely to have other confounding conditions such as OSA, suggesting that the crash risk is not solely due to diabetes. In the USA, patients with insulin-requiring diabetes are not allowed to drive commercially, except under stringent waiver criteria. The link of diabetes and crashes itself has been questioned by the latest report by the FMCSA examining evidence from the medical expert panel.1 Laberge-Nadeau et al9 suggested that the lack of consistent association between crash risk and diabetes in commercial drivers may be due to ‘healthy worker effect’. Diabetes treatment, with oral hypoglycaemic agents but not with insulin, was found to be associated with crashes.9 ,38 This may be explained by drivers using varying diets at times (trying to pass the examination) or by inaccurate reporting of the type of medication they use.
Drugs and alcohol misuse, not a rare problem in the general population, is under-reported in commercial drivers.52 In the absence of regular and random drug testing surveillance, this low incidence is likely due to under-reporting because of fear of losing certification.
Engaging employees in the development and execution of interventional programmes is one approach that was found to be helpful. The use of programs such PeerCare alcohol program47 and BP DownShift program,31 ,44 for hypertension management showed not only health benefits but also provided evidence for how employees are capable of lowering healthcare costs.
The presence of concomitant medical conditions is thought to be associated with a higher risk of crashes.25 This increased risk can be attributed to complications of the comorbid conditions (cardiovascular event) or due to aggressive management of conditions by drivers in fear of losing their license, which can increase the burden of treatment, side effects and drug interactions.
The type of vehicle is another factor that may affect how comprehensive or detailed the medical examination should be. The severity of crashes varies between vans, trucks and buses. Bus accidents have been found to be more severe, linked with more deaths and possess a greater public safety hazard. There has been a call for stricter regulations to qualify bus drivers.12
There is paucity of evidence when it comes to diagnosis of medical conditions in commercial drivers. Thus, diagnostic evidence is derived from the general population. The prevalence of certain conditions may be different in commercial drivers, thus affecting the diagnostic accuracy of the tests. Some studies found a single diagnostic test to be sufficient,25 ,37 ,39 ,43 whereas a systematic review by Marino et al13 concluded that single screening tests cannot be used to evaluate fitness-to-drive. This review highlighted the lack of evidence to support the use of existing clinical and neuropsychological screening tests and called for developing and validating new tests for drivers with chronic conditions. In addition, there is paucity of evidence regarding the relationship between health conditions and crash risk and the best way to evaluate which drivers are safe with a given condition and which are not.
This systematic review has several limitations. The different designs of included studies made in attempts to reduce heterogeneity statistically implausible. Many of the studies are cross-sectional which limits inference and establishing causality. Even in the cohort studies, the lack of concrete definition of healthy controls and the selection of higher risk groups might cause bias. We were unable to test for publication and reporting biases, which are likely when dealing with observational studies that do not require prior registration. It is possible that we have missed some relevant studies considering the lack of specific indexing terms for commercial driving and the varying terminology of the fitness-to-drive examination.
The available evidence provides rationale for the medical evaluation of commercial drivers but does not clearly dictate what type of examination is needed to determine fitness-to-drive. There is a clear increased prevalence of important health conditions in commercial drivers and there is a correlation of some of these conditions with crashes. Randomised trial design in this setting is challenging and is neither practical nor ethical. In addition, several high-risk and chronic conditions that are relevant to the fitness to drive are under-reported in the literature, including visual impairments, epilepsy, sexually transmitted diseases, the use of illicit drugs and kidney diseases. The implementation of in-motion naturalistic studies and interventional programmes such as Ticketing Aggressive Cars and Trucks (TACT) is attainable and carries a solution to assessing and educating on-duty drivers.7 ,53 ,54 Undoubtedly, there is a substantial need to qualify medical personnel to examine and certify drivers for fitness-to-drive. Tailored and occupational health certification courses should not be delayed and currently rank in high priority. The upcoming 2013-14 FMCSA guidelines in the USA may provide some support to such recommendation. There is also a need to establish the importance of individual case-to-case assessment and to avoid advertising one-rule-fits-all, as a physician's discretion remains valuable.
Individual and public education programmes may also be helpful. Commercial drivers-specific assessment training programmes to educate and certify specialised cadres are recommended. The need for further research in assessing diagnostic tests and examining other challenging diagnoses is of importance. Efforts to engage all stakeholders including drivers, employers, unions, physicians and guiding agencies are much needed to achieve these goals.
In conclusion, several medical conditions are highly prevalent in commercial drivers and some of them are associated with increased risk of crashes, thus providing a rationale for requiring medical evaluation of commercial motor vehicle drivers. However, the current evidence is insufficient to recommend diagnostic strategies specific to commercial drivers that can be implemented in current occupational practice, and these strategies are currently derived from studies in the general population.
REFERENCES
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Footnotes
-
Contributors All authors have contributed substantially the body of work and fulfilled the ICMJE guidelines to grant a coauthorship. All authors have given final approval of this version to be published. AMAD participated in study codesigning, data collection and screening, data-analysis and evidence synthesis, and drafting and revising the manuscript. BF participated in study codesigning, data collection and screening, evidence-synthesis and codrafting the manuscript. CTC participated in part of the experts’ panel in hypothesis generation, data analysis and revising the manuscript. LWS participated in part of the experts’ panel in hypothesis generation and design, data analysis, and revising the manuscript. LJP participated in data acquiring, literature search and screening and revising the manuscript. MHM participated in part of the experts’ panel in hypothesis generation and design, data analysis and synthesis and codrafting and revising the manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.