Article Text

Abstract
Background Poor cardiorespiratory fitness is associated with cardiovascular disease risk factors.
Aim To perform a systematic review and meta-analysis of the relationship between poor cardiorespiratory fitness and cardiovascular disease risk in children and adolescents.
Methods Systematic literature search (1980 to 11 April 2015) for studies that determined a cardiorespiratory fitness cut point that predicted cardiovascular disease risk in children and adolescents.
Results We identified 7 studies that included 9280 children and adolescents (49% girls) aged 8–19 years from 14 countries. Cardiovascular disease risk was already present in boys (6–39%) and girls (6–86%). Boys with low fitness (<41.8 mL/kg/min) had a 5.7 times greater likelihood of having cardiovascular disease risk (95% CI 4.8 to 6.7). The comparable diagnostic OR for girls with low fitness (<34.6 mL/kg/min) was 3.6 (95% CI 3.0 to 4.3). The 95% confidence region of cardiorespiratory fitness associated with low cardiovascular disease risk ranges, 41.8–47.0 mL/kg/min in boys (eg, stages 6–8 for a boy aged 15 years) and 34.6–39.5 mL/kg/min in girls (eg, stages 3–5 for a girl aged 15 years). The cardiorespiratory fitness cut point to avoid cardiovascular disease risk ranged 41.8 mL/kg/min in boys and was 34.6 mL/kg/min in girls.
Summary Fitness levels below 42 and 35 mL/kg/min for boys and girls, respectively, should raise a red flag. These translate to 6 and 3 stages on the shuttle run test for a boy and a girl, both aged 15 years, respectively. These cut points identify children and adolescents who may benefit from primary and secondary cardiovascular prevention programming.
- Aerobic fitness
- Children
- Adolescent
- Cardiovascular
- Exercise testing
Statistics from Altmetric.com
Introduction
Cardiovascular disease is the leading cause of global mortality. The precursors of cardiovascular disease have its origin in childhood.1 Cardiovascular disease risk factors during childhood and adolescence are associated with more extensive fatty streaks and fibrous plaques in adults,1 with artery calcification in young adults2 and with common artery intima media thickness in adulthood.3 The most recognised cardiovascular disease risk factors in children and adolescents are triglycerides, total cholesterol (TC), high-density lipoprotein cholesterol (HDL), insulin, glucose, waist circumference and blood pressure.4–8
Cardiorespiratory fitness reflects (1) the overall capacity of the cardiovascular and respiratory systems and (2) the ability to carry out prolonged, rhythmic and dynamic exercise involving large muscles of the body.9 It is a direct measure of aerobic functional capacity. There is an unequivocal association between poor cardiorespiratory fitness and cardiovascular disease risk factors in children and adolescents.10 Children and adolescents with low cardiorespiratory fitness have higher risk of cardiovascular disease11 and myocardial infarction during adulthood.12 Children and adolescents with low cardiorespiratory fitness also have low fitness levels years later.13
Cardiorespiratory fitness has historically been included in almost all children and adolescents fitness test batteries.14 Cardiorespiratory fitness test scores were originally tracked as a marker of performance, but the increasing focus on health-related fitness has led to its use as a screening test to identify children and adolescents at increased risk of cardiovascular disease.15–17 The Fitnessgram program in the USA has even used the fitness criterion-referenced standards to provide individualised feedback on cardiovascular risk on student reports; this is uncommon in other countries. Although fitness is widely used in schools and children and adolescents programming, clinicians or other health agencies that evaluate present or future cardiovascular disease risk at these ages have not adopted these standards.
Three barriers to health professionals/public health adopting fitness testing to evaluate health are the lack of standardisation in (1) the test protocols and (2) the health outcomes being evaluated, as well as (3) the absence of evidence-based clinical cut points at these ages. To facilitate fitness testing to assess cardiovascular disease risk in clinical settings and in schools, it is important to work towards international standards similar to those developed for body composition.18
Thus, the aim of this meta-analysis was to systematically evaluate the relationship between low cardiorespiratory fitness and cardiovascular disease risk in children and adolescents from several countries. Specifically, we addressed the question: are there cardiorespiratory fitness cut points associated with cardiovascular disease risk in children and adolescents? The goal was to identify what fitness level should raise a red flag. We aimed to provide pooled fitness cut points that could serve as standards for international comparisons and for clinical applications.
Methods
Search strategy and study selection
We followed the checklist of the Meta-analysis of Observational Studies in Epidemiology19 and the recommendations of the Cochrane Collaboration Handbook.20 We conducted a systematic literature search of MEDLINE, EMBASE, The Cochrane Library, Web of Science and SPORTDiscus (1980 to 11 April 2015) for studies that determined the cardiorespiratory fitness cut point associated with cardiovascular disease risk. We combined three search topics using the Boolean operator AND. The first key words were related to children and adolescents as follows: ‘adoles* OR child* OR schoolchildren’. The second key words were related to cardiorespiratory fitness: ‘cardiorespiratory fitness OR cardiovascular fitness OR aerobic capacity OR aerobic fitness OR maximal oxygen consumption OR VO2max OR VO2peak’. The third keywords were related to the outcome of this meta-analysis: ‘cardiovascular disease OR cardiovascular disease risk OR cardiovascular health OR metabolic syndrome OR metabolic risk OR cardiometabolic risk OR insulin resistance OR dyslipidemia OR hypertension OR blood pressure OR diabetes mellitus’. In addition, we searched the reference lists of all identified relevant publications.
Inclusion criteria
Two reviewers (IC-R and JRR) independently examined the title and abstract of each reference to identify those studies that were likely to report the cardiorespiratory fitness (VO2max, mL/kg/min) cut point and then obtained the full text. Disagreements about study selection were resolved by consensus with a third reviewer (VM-V). The full text was retrieved for articles that could not be excluded based on title and abstract to determine final inclusion.
We included studies if: (1) the age range of participants was between 8 and 19 years; (2) data were reported by sex; (3) cardiorespiratory fitness was assessed by a submaximal or maximal exercise test and can be expressed as VO2max (mL/kg/min); (4) a cardiorespiratory fitness cut point associated with cardiovascular disease risk was calculated in the study; (5) at least two cardiovascular disease risk factors were measured and (6) definition of cardiovascular disease risk are provided. No restrictions were considered regarding study design (cross sectional, case–control, cohort study) or data collection (prospective or retrospective).
To avoid duplicate data, we identified articles that included the same group of participants by reviewing interstudy similarity in any of the following characteristics: country in which the study was conducted, investigators who performed the study, source of patients, recruitment period and inclusion criteria. When the same investigators reported results obtained on the same group of patients in several publications, only the largest series was included in the analysis.
Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) criteria21 were used to standardise the assessment of the quality of the included studies. This 7-item tool has been proposed for the quality evaluation of included studies in meta-analyses of diagnostic accuracy and categorises the risk of bias and the study generalisability as low, unclear or high. Both reviewers scored independently the seven items of QUADAS-2 (IC-R and JRR), and disagreements were resolved via consensus with a third reviewer (VM-V).
Data extraction and synthesis
Two authors (IC-R and JRR) independently reviewed each published study and extracted the following information: first author's name, year of publication, study name, country of origin, cardiovascular disease risk factors, definition of cardiovascular disease risk, cardiorespiratory fitness test used to estimate VO2max, participants' sex and age, number of participants, cardiorespiratory fitness cut points associated with cardiovascular disease risk, prevalence of cardiovascular disease risk, sensitivity, specificity and area under the curve (AUC). Any disagreement was resolved by consensus with a third reviewer (VM-V).
Statistical analyses
The diagnostic OR (dOR) was computed by the Moses’ constant of linear model and in the context of a random effects model. This approach relies on the linear regression of the logarithm of the dOR of a study (dependent variable) on an expression of the positivity cut point of that study (independent variable).22 The dOR is a single indicator of test accuracy that combines the sensitivity and specificity data into a single number.11
Study heterogeneity was assessed with an I2 statistic. A large I2 value indicates that data are not consistent with a simple pooling model; a more sophisticated model is needed to properly combine the data. Accordingly, a random-effects model based on the Der Simonian and Laird method was used to model test performance and account for heterogeneity among studies not attributable to observed study characteristics. Cardiorespiratory fitness (VO2max) test performance in the presence of heterogeneity was summarised using hierarchical summary receiver operating curves (HSROC).23
The influence of each independent study in the pooled estimates of dOR was detected by sensitivity analysis. For assessing the potential publication bias, we used the funnel plot proposed by Deeks et al,24 which visually assess publication bias by using a scatter plot of the inverse of the square root of the effective sample size (1/ESS1/2) versus the diagnostic logit dOR (logdOR), which should have a symmetrical funnel shape when publication bias is absent. The degree of asymmetry in the plot was statistically evaluated by a regression of the logit dOR against 1/ESS1/2, weighted by ESS. Additionally, the pooled sensitivity, specificity, positive likelihood ratio (PLR) and negative likelihood ratio (NLR) for cardiorespiratory fitness (VO2max) test (pooled across studies) and their 95% CIs were calculated.25
All analyses were undertaken using STATA V.13.0 (STATA Corp, College Station, Texas, USA).
Results
Literature search and study characteristics
Figure 1 shows the number of studies that were identified and excluded at different stages of the selection process. Seven studies were included in the present meta-analysis,17 ,26–31 including 9280 children and adolescents (4717 boys and 4563 girls) aged 8–19 years from 14 countries (table 1). The list of cardiovascular disease risk factors measured in the included studies and the definition of cardiovascular disease risk are shown in table 1. One study did not provide the prevalence of cardiovascular disease risk28 in girls, and two studies provided information for two different age groups.29 ,30 The prevalence of cardiovascular disease risk ranged from 6% to 39% in boys and from 6% to 86% in girls.
Characteristics of studies included in the meta-analysis
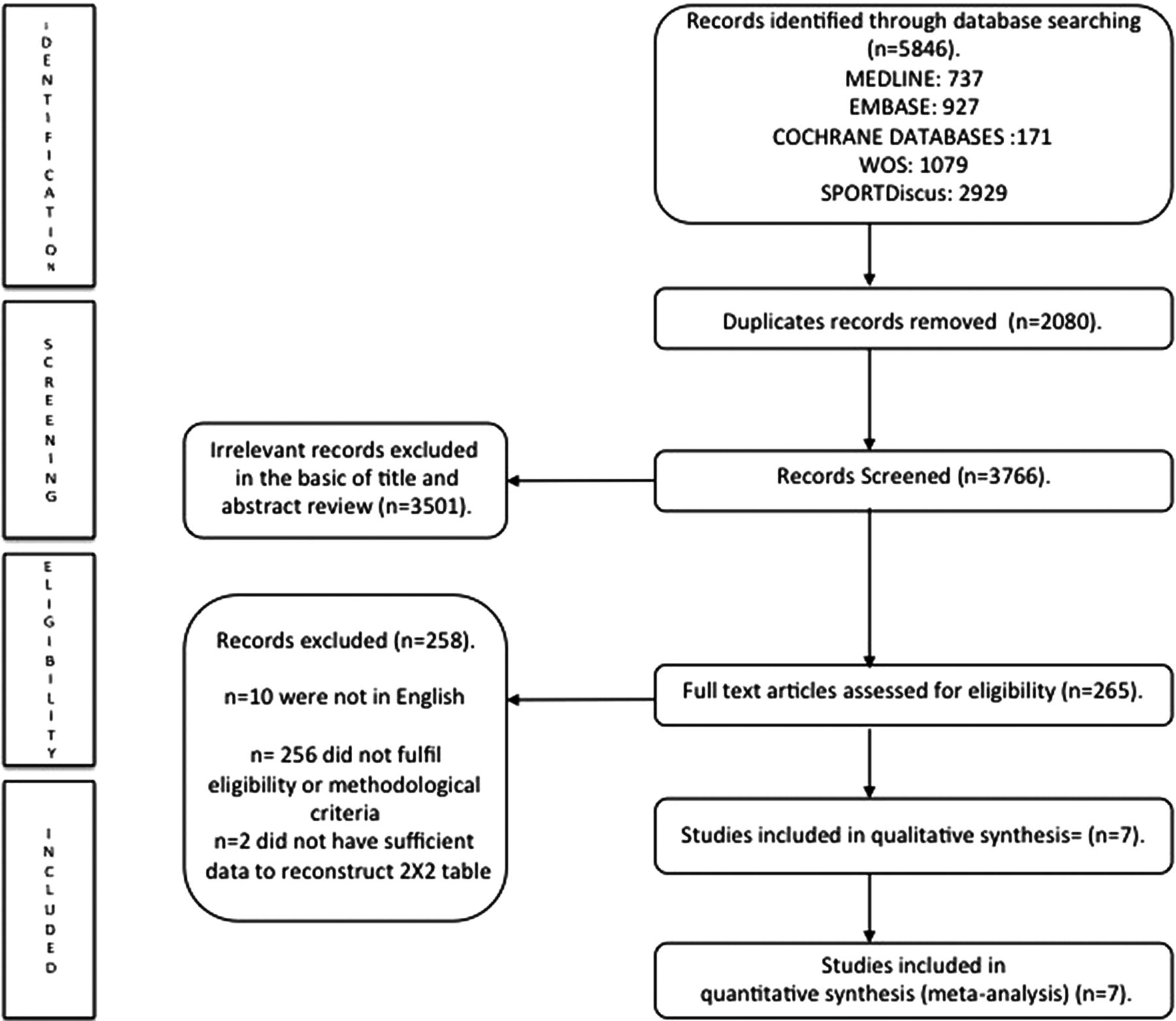
Selection of articles for meta-analysis.
Study quality
All included studies were assessed as low risk of bias in terms of both domains of the QUADAS-2 tool, the reference standard and flow and timing criteria. One study scored high risk of bias in terms of the index test (VO2max).24 One study was rated as unclear risk of bias in selection of participants' criterion.29 Three studies scored unclear concerns regarding applicability in participants' selection,31 ,37 ,38 and six studies were rated as unclear concerns regarding applicability in the index test28 ,31 ,37–39 (see online supplementary figure S1).
Supplementary figure
Meta-analysis
Table 2 shows the pooled sensitivity, specificity, PLR, NLR, dOR and AUC estimates for boys and girls. Overall, the pooled sensitivity estimates for cardiorespiratory fitness were 65.0 (95% CI 60.0 to 71.0) for boys and 60.0 (95% CI 56.0 to 65.0) for girls, and the pooled specificity estimates were 77 (95% CI 74 to 80) for boys and 74 (95% CI 72 to 77) for girls. Moreover, the pooled PLR and NLR for boys were 2.81 (95% CI 1.18 to 6.70) and 0.39 (95% CI 0.17 to 0.92), respectively, and for girls these estimates were 2.05 (95% CI 0.78 to 5.39) and 0.44 (95% CI 0.17 to 1.14), respectively. What do these results mean given a 20% prevalence of cardiovascular disease (200/1000)? Boys and girls with fitness levels falling in the healthy ranges (see below) have a probability of 89.9% and 88.2%, respectively, of not having cardiovascular disease risk.
Summary of the pooled accuracy parameters analysis for cardiorespiratory fitness by sex
Figure 2 displays the forest plots of dOR by sex. An unadjusted pooled analysis of the studies showed evidence of significant heterogeneity among studies in boys dOR (I2 of 66%) and in girls dOR (I2 of 79%). The pooled dOR estimates were 5.7 (95% CI 4.8 to 6.7) for boys and 3.6 (95% CI 3.0 to 4.3) for girls, which indicates that boys with low fitness (<41.8 mL/kg/min) had a 5.7 times greater likelihood of having cardiovascular disease risk compared to those with the fitness level equal or higher than 41.8 mL/kg/min. Similarly, girls with low fitness (<34.6 mL/kg/min) had a 3.6 times greater likelihood of having cardiovascular disease risk compared to those with the fitness level equal or higher than 34.6 mL/kg/min. Additional forest plots and pooled accuracy parameters are provided in online supplementary figures S2–S5.

Pooled estimates dOR forest plot by sex. (A,B) Different subgroups of participants in that study, as defined by setting (table 1). dOR, diagnostic OR.
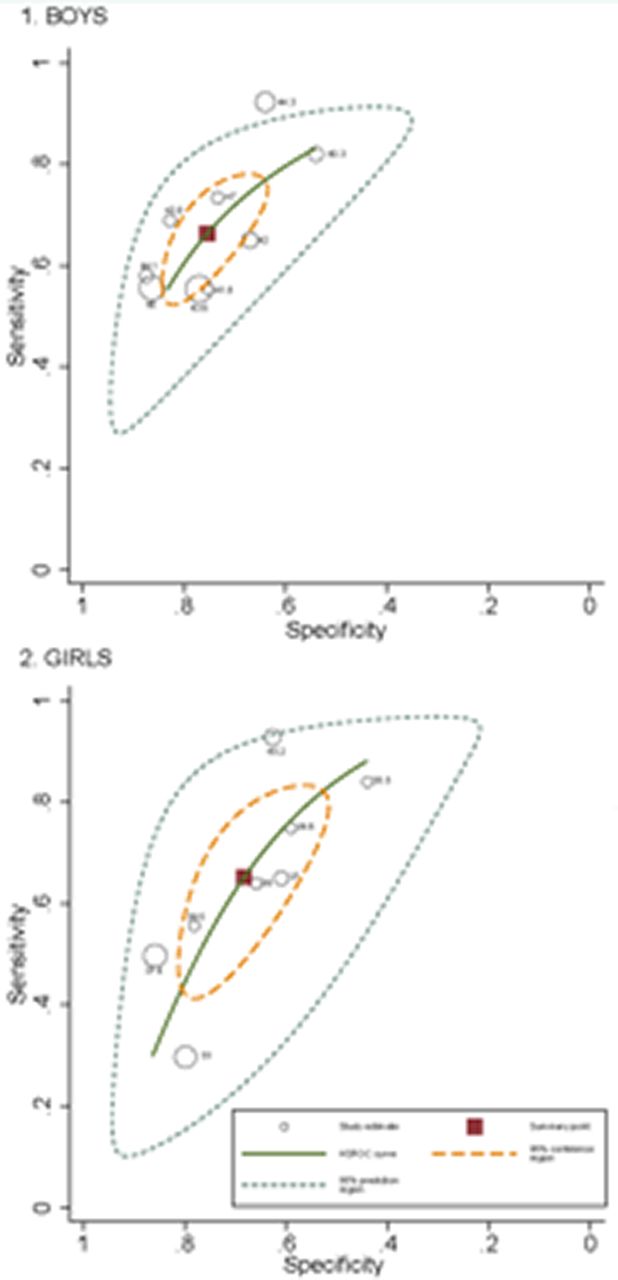
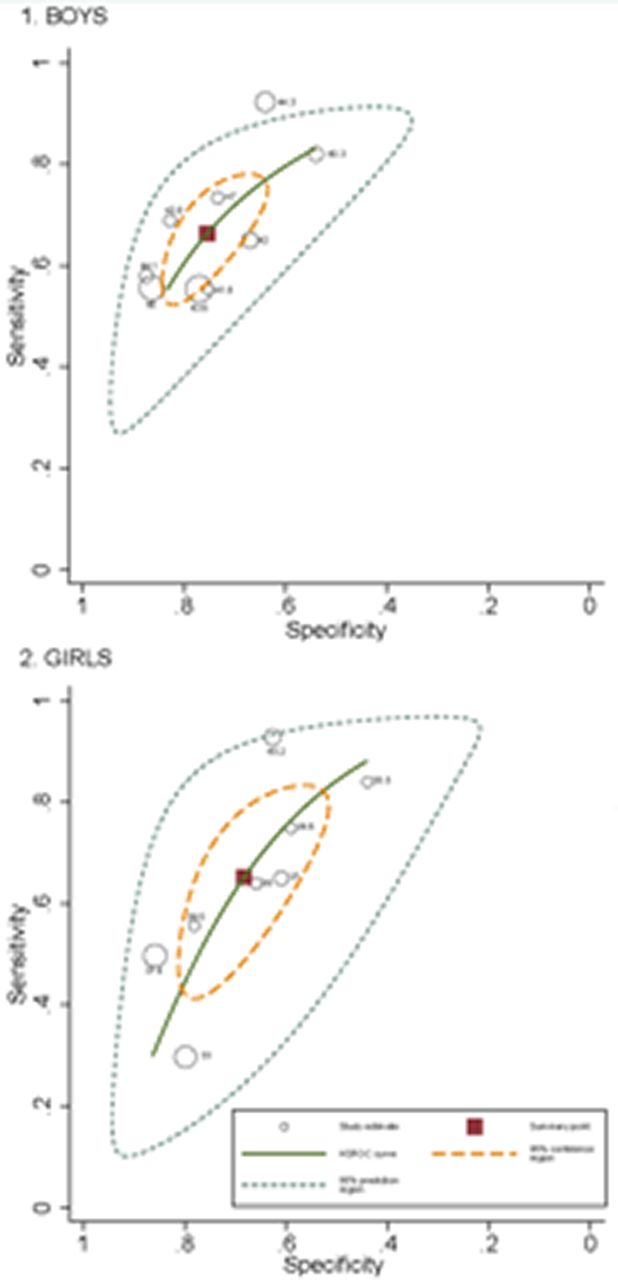
The area under the HSROC curve estimating the discriminating accuracy of cardiorespiratory fitness for identifying cardiovascular disease risk was 0.71 (95% CI 0.65 to 0.76; p<0.001) in boys and 0.64 (95% CI 0.58 to 0.69; p<0.001) in girls (figure 3).
{kind=link}
{kind=link}
{kind=link}
HSROC curve summarising the potential of cardiorespiratory fitness to identify cardiovascular disease risk by sex. The 95% confidence region for the summary point included studies in which the cut point for cardiorespiratory fitness ranged from 41.8 to 47.0 mL/kg/min in boys and between 34.6 and 39.5 mL/kg/min in girls. HSROC, hierarchical summary receiver operating characteristic.
The 95% CI region for the summary point included studies in which the cut point for cardiorespiratory fitness ranged from 41.8 to 47.0 mL/kg/min in boys and between 34.6 and 39.5 mL/kg/min in girls.
Sensitivity analyses and publication bias
Sensitivity analyses revealed that no studies unduly influenced the pooled estimates of dOR in boys. However, in girls, the pooled dOR estimates changed after removing data of both age group samples of the study by Adegboye et al;30 when removed the 8–11 years old group, the dOR worsened (dOR=3.0; 95% CI 2.4 to 3.7), and when the 14–17 years old group was removed, it improved (dOR=4.4; 95% CI 3.6 to 5.3) (see online supplementary figure S6).
The Deek's funnel plot displayed a symmetric distribution of the points corresponding to each study (boys: intercept, 0.87; 95% CI −0.49 to 2.23; p=0.175; girls: for intercept, 0.55; 95% CI −1.40 to 2.50; p=0.515), indicating that publication bias was unlikely (see online supplementary figure S7). None of the included studies reported any adverse event.
Discussion
The present meta-analysis documents the robust utility of cardiorespiratory fitness as a predictor of cardiovascular disease risk in children and adolescents. The consistency of findings across countries supports the cross-cultural generalisability of these associations. Indeed, stability across studies is especially noteworthy considering inherent differences in (1) fitness test protocols (eg, laboratory and field-based tests, submaximal and maximal-effort tests), (2) prediction equations used to estimate cardiorespiratory fitness, (3) cardiovascular disease risk factors measured and (4) definitions of cardiovascular disease risk (table 1). This reinforces the existence of generalised cardiorespiratory fitness cut points associated with cardiovascular disease risk in children and adolescents.
Cardiovascular disease risk-related cut points
The fitness cut points to avoid cardiovascular disease risk fell between 41.8 and 47.0 mL/kg/min in boys aged 8–17 years and between 34.6 and 39.5 mL/kg/min in girls aged 8–17 years. In a hypothetical scenario of a population with a 20% prevalence of cardiovascular disease risk (200/1000), boys and girls with healthy fitness levels have a probability of 89.9% and 88.2%, respectively, of not having cardiovascular disease risk.
We found that the cardiorespiratory fitness cut point associated with cardiovascular disease risk was around 12 metabolic equivalents (12 METs, 42 mL/kg/min) for boys and 10 (10 METs, 35 mL/kg/min) for girls. Interestingly, the empirically derived values are similar to those used originally to identify fit versus unfit adolescents in the 90's by the Fitnessgram health-related fitness battery. They suggested a cardiorespiratory cut point of ≥38 and ≥42 mL/kg/min for girls and boys, respectively,40 which were extrapolated from the adults' cut points associated with a higher risk of mortality. The current Fitnessgram standards vary across age to take growth and maturation into account,17 but those fall within the same ranges highlighted here. These same standards also have similar predictive utility for detecting risk of metabolic syndrome in a nationally representative sample of Hungarian youth. In that study, youth who were unfit (23% of boys and 43% of girls) were 2.8 times more likely to have metabolic syndrome than their fit counterparts. These findings further document the cross-cultural generalisability of the cut points.41
Translating cardiorespiratory fitness standards into units that can influence public health
With the widely used 20 m shuttle run test,42 ,43 the achievement of the health-related fitness cut point can be easily determined using age-specific and gender-specific tables (see table 3). To achieve the cardiorespiratory fitness cut points to avoid cardiovascular disease risk, a boy aged 15 years and a girl aged 15 years should run at 11 km/hour (stage 6) and 9.5 km/hour (stage 3), respectively. Cardiorespiratory fitness as measured by this test has already been considered a relevant marker of current health,10 as well as an indicator of future cardiovascular health.11 It has been used in more than one million children and adolescents from about 50 countries.43 Moreover, the test is used as the basis for personalised fitness reports in the USA and was endorsed by the National Academy of Medicine as an indicator of cardiorespiratory fitness for public health surveillance.38 Of note is also that the test has a good validity,14 and reliability,44 and it is feasible and safe37 for the assessment of cardiorespiratory fitness in children and adolescents. It is recommended to be used for health monitoring purposes at population level,15 as well as in the school setting. The 20 m shuttle run test (with minimal adaptations) is also reliable and valid in children as young as 3–5 years old.38 ,39 This test is part of the evidence-based ALPHA-fitness test battery for children and adolescents.15
Twenty meter shuttle run stages that need to be met to fall within the healthy cardiorespiratory fitness level by age and gender
Cardiorespiratory fitness and current and future youth's health
Findings from cross-sectional studies have shown that low cardiorespiratory fitness is not only associated with higher cardiovascular disease risk but also with decreased mental and skeletal health.10 ,45 Moreover, data from longitudinal studies indicate that there is strong evidence that low cardiorespiratory fitness in childhood and adolescence is a predictor of cardiovascular disease risk later in life.11 Poor cardiorespiratory fitness in childhood and adolescence has also been associated with higher risk of metabolic syndrome,46 arterial stiffness47 ,48 and myocardial infarction years later.12 Levels of cardiorespiratory fitness tend to track from childhood to adolescence,49 ,50 as well as from adolescence to adulthood.13 ,51 Taken together, these findings support the notion that the promotion of high cardiorespiratory fitness levels should start at childhood.13
Settings to assess and improve fitness
Schools as well as sport clubs might be a convenient setting to promote a healthy lifestyle among young populations.52 Schools could collect this information to encourage children to be more physically active to achieve and go beyond the suggested cardiorespiratory fitness cut points.53 While this evaluation might not provide diagnoses per se, it could serve as screening element to identify young people with cardiovascular disease risk who might benefit from intervention programmes. Moreover, such screening can be used as a tool to teach youth about how to monitor and improve their fitness. Schools can play a leadership role to promote physical activity and health,53 as well as to combat poor fitness among youth. There are indeed good examples on what can be performed at the school setting: McDonald and Trost54 evaluated the efficacy of a school-based goal setting and self-monitoring intervention on aerobic fitness in middle school students and showed a significant increase in aerobic fitness over the 10-week period, whereas fitness levels among students participating in their usual school physical education declined. We suggest that children should be tested in physical education lessons using a cardiorespiratory field test, if possible every year. Testing could be used as a pedagogical tool for the physical education teacher to help children with poor fitness, as well as to keep encouraging being physically active to those with high fitness levels.
There are several examples of good practice in terms of monitoring body weight status and fitness among young US citizens.55 Unfortunately, despite the relevant information provided by a relatively simple assessment of cardiorespiratory fitness, such data rarely become available or are not used by public health and clinical practitioners for purposes of health promotion or disease prevention.29 Physicians have access to measures of cardiovascular disease risk factors such as fasting blood samples and blood pressure; however, some of these procedures are invasive, expensive and not suitable for cardiovascular disease risk screening among large populations of children and adolescents and at school settings. The origins of cardiovascular disease are found in childhood,1 and low cardiorespiratory fitness levels at childhood and adolescence are associated with cardiovascular disease risk during these years and later in life;10 ,11 thus, lifestyle modification focused on enhancing physical activity and increasing fitness might help improving their cardiovascular health.
Strengths and limitations
The findings from the present study support the cross-cultural generalisability of the cardiorespiratory fitness standards in children and adolescents, but there are some limitations of this meta-analysis that should be considered. Some of them are common to meta-analyses (eg, publication bias, selection bias and limited information from study reports). Even though we did not find evidence of significant publication bias, this does not completely exclude this possibility. The results showed substantial level of heterogeneity, thus should be interpreted with caution. The total number of studies in our analyses was relatively small; however, this may be offset by the inclusion of a relatively large number of children and adolescents (n=9280). In addition, available studies are restricted to 14 countries including a representative sample of USA, as well as countries from Europe with diverse environmental, cultural and social factors. It would be desirable to have data from other geographical locations to make the results generalisable to all populations around the globe. Unfortunately, there are not enough studies to conduct analyses by age group, nevertheless we have conducted a sensitivity analysis excluding studies that included children aged under 12 years, and the estimations did not change substantially. VO2max associated with a healthier cardiovascular profile ranged from 43.8 to 47.0 mL/kg/min in boys and from 33.0 to 36.0 mL/kg/min in girls older than 12 years.
Next steps
On the basis of our meta-analysis, we suggest four steps.
Development of a cardiovascular prediction algorithm in paediatric populations (eg, International Diabetes Federation) that consider cardiorespiratory fitness and the traditional cardiovascular disease risk factors to allow paediatricians to use cardiorespiratory fitness as a way of stratifying risk in clinical settings. Currently, the International Diabetes Federation does not even include cardiorespiratory fitness in the definition of metabolic syndrome, which might be interpreted that fitness is not an important parameter of metabolic health. The present study suggests otherwise and provides health-related cut points that could be used;
Evaluation of feasibility of exercise testing for assessing cardiorespiratory fitness in the schools, sport clubs56 or clinical settings from the viewpoint of primary prevention of cardiovascular disease;
Long-term longitudinal studies testing whether children and adolescents meeting the cardiorespiratory fitness cut points have a better cardiovascular health later in life, and lower risk of developing cardiovascular disease;
A clinical trial to determine whether an exercise-based intervention that improves cardiorespiratory fitness also improves the cardiovascular profile and prevents future cardiovascular disease, including metabolic syndrome, type 2 diabetes, obesity or hypertension.
Conclusions
Our meta-analysis suggests that cardiorespiratory fitness, which can be easily assessed by a field-based exercise test (ie, the 20 m shuttle run test), can be used as a marker of cardiovascular health in children and adolescents. On the basis of the results presented here, fitness levels below 42 and 35 mL/kg/min for boys and girls, respectively, should raise a red flag. The consistency of findings reported in the present study provide strong evidence to support the broader adoption of cardiorespiratory fitness standards for use in schools and sport programmes as well as in clinical settings as part of surveillance and/or screening systems to identify children and adolescents with cardiovascular disease risk who might benefit from intervention programmes.
What are the findings?
Cardiorespiratory fitness is a marker of cardiovascular health in children and adolescents.
Cardiorespiratory fitness cut points to avoid cardiovascular disease risk range between 41.8 and 47.0 mL/kg/min in boys and between 34.6 and 39.5 mL/kg/min in girls.
References
Footnotes
Contributors JRR and VM-V had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. They are also responsible for study concept and design. JRR, IC-R and VM-V contributed to acquisition of data and statistical analysis. JRR, IC-R, GJW, LBA, FBO and VM-V involved in the analysis and interpretation of data and critical revision of the manuscript for important intellectual content. JRR, IC-R, LBA and VM-V involved in the drafting of the manuscript.
Funding JRR and FBO are recipients of a Ramón y Cajal Fellowship by the Spanish Ministry of Economy and Competitiveness (grants RYC-2010-05957 and RYC-2011-09011, respectively) and by the University of Granada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available in the tables.