Article Text

Abstract
Objective Temporal changes in the healthcare burden of atrial fibrillation (AF) are less well known in rapidly ageing Asian countries. We examined trends in hospitalisations, costs, treatment patterns and outcomes related to AF in Korea.
Methods Using the National Health Insurance Service (NHIS) database involving the entire adult Korean population (n=41 701 269 in 2015), we analysed a nationwide AF cohort representing 931 138 patients with AF. We studied all hospitalisations due to AF from 2006 to 2015.
Results Overall, hospitalisations for AF increased by 420% from 767 to 3986 per 1 million Korean population from 2006 to 2015. Most admissions occurred in patients aged ≥70 years, and the most frequent coexisting conditions were hypertension, heart failure and chronic obstructive pulmonary disease. Hospitalisations mainly due to major bleeding and AF control increased, whereas hospitalisations mainly due to ischaemic stroke and myocardial infarction decreased. The total cost of care increased even after adjustment for inflation from €68.4 million in 2006 to €388.4 million in 2015, equivalent to 0.78% of the Korean NHIS total expenditure. Overall in-hospital mortality decreased from 7.5% in 2006 to 4.3% in 2015. The in-hospital mortality was highest in patients ≥80 years of age (7.7%) and in patients with chronic kidney disease (7.4%).
Conclusions AF hospitalisations have increased exponentially over the past 10 years in Korea, in association with an increase in comorbid chronic diseases. Mortality associated with AF hospitalisations decreased during the last decade, but hospitalisation costs have markedly increased.
- atrial fibrillation
- health care economics
- quality and outcomes of care
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia in the general population, and is associated with increased mortality and morbidity.1 The number of persons with AF has been projected to increase to 12.1–15.9 million in the USA by 2050 and 17.9 million in Europe by 2060, with more than half of these patients ≥80 years of age.2–4 Consequently, the healthcare burden of AF is growing considerably, and is mainly related to hospitalisations.5–7 The total cost related to AF care was estimated as US$6–US$26 billion in the USA and it accounts for 1% of the national healthcare budget in the UK.5–7
While the global burden of AF has increased over recent decades, most studies about the epidemiology and care burden of AF are based on the predominantly white populations of North America or Europe.8 The actual disease burden of AF in Asia is rapidly increasing given the larger proportional increase in the elderly population.9 10 However, the impact of AF on hospitalisations and mortality, and the economic burden of AF is less understood in Asian populations. A nation-level study of the temporal trends in healthcare burden of AF is essential for establishing the burden of AF and appropriate healthcare planning. Therefore, we used a national insurance database to evaluate a contemporary AF-related hospital care burden. We examined temporal trends in hospitalisations, the effects of comorbid diagnoses, costs, treatment patterns and outcomes related to AF in Korea.
Methods
Data sources
This study is based on the national health claims database established by the National Health Insurance Service (NHIS) of Korea.11 The NHIS is the single insurer managed by the Korean government, and the majority (97.1%) of the Korean population are mandatory subscribers, while the remaining 3% of the population are medical aid subjects. The NHIS database contains information on medical aid subjects as well; therefore, it is based on the entire Korean population. The following medical information is provided: sociodemographic information, patient use of inpatient and outpatient services, pharmacy dispensing claims and mortality data. Every population in the NHIS database was linked by Korean social security numbers, and all social security numbers were deleted after constructing the cohort by using serial numbers to prevent leakage of personal information. These databases are open to researchers, whose study protocols are approved by the official review committee. Informed consent was waived.
Study population
Between 1 January 2006 and 31 December 2015, 931 138 patients with AF were identified from the entire Korean population. AF was diagnosed using the International Classification of Disease 10th Revision (ICD-10) codes I48 (AF and atrial flutter), I48.0 (AF) and I48.1 (atrial flutter). To ensure diagnostic accuracy, patients were defined as having AF only when it was a discharge diagnosis or confirmed more than twice in the outpatient department.12–17 Diagnosis of AF has previously been validated in the NHIS database with a positive predictive value of 94.1%.15 17 Patients aged <20 years or with valvular AF (with a diagnosis of either mitral stenosis (ICD-10: I05.0, I05.2 and I34.2) or prosthetic heart valves (ICD-10: Z95.2–Z95.4) or insurance claims for valve replacement or valvuloplasty) were excluded.
All hospitalisations due to AF from 2006 to 2015 and the cost of each inpatient stay were studied. AF hospitalisations and inpatient costs were obtained in two different ways: 1) overall AF hospitalisation (AF as any diagnosis of up to five discharge diagnoses) and 2) AF hospitalisation due to each main cause including major bleeding, ischaemic stroke, AF control (AF as principal discharge diagnosis), myocardial infarction (MI), heart failure, sick sinus syndrome (SSS) or pacemaker (PM) related, and radiofrequency catheter ablation (RFCA) for AF. All costs were calculated in Korean won (KRW) and converted into Euros (1 EUR=1282.7 KRW). Cost was adjusted for inflation by calculating in terms of the 2015 cost using the Korean Consumer Price Index data.18
Comorbidities, economic status and medications
Comorbidities were defined using medical claims according to ICD-10 codes and prescription medication use. To ensure diagnostic accuracy, patients were considered to have comorbidities when it was a discharge diagnosis or was confirmed more than twice in an outpatient setting, similar to previous studies with the NHIS.12 13 15–17 The definitions of comorbidities and main hospitalisation causes are presented in online supplementary table 1. Economic status variables were categorised into three groups based on the total amount of national health insurance premiums paid by an insured person in each year, which is proportional to the person’s income: low, intermediate and high economic status. Prescription medication use was ascertained by identifying NHIS database claims. Medication use among patients with AF in a given year was defined when the medication was prescribed for >180 days in the particular year.
Supplementary file 1
Statistical analysis
AF hospitalisations are presented as numbers per 1 million Korean population and as numbers per 100 patients with AF in a given year. Hospitalisations per 1 million Koreans were the number of hospitalisations in a given year divided by the total number of Korean residents who were alive in that year. Online supplementary table 2 shows the number and distribution of total Korean residents aged ≥20 years. Hospitalisations per 100 patients with AF were the number of hospitalisations in a given year divided by the total number of Korean patients with AF in that year and multiplied by 100. The Cochran-Armitage trend test was used to analyse temporal trends of categorical variables. For continuous variables such as hospitalisation costs, the non-parametric test for trends by Jonckheere-Terpstra was used. All tests were two-tailed, with P<0.05 considered to be statistically significant. Statistical analyses were conducted with SAS V.9.4 (SAS Institute, Cary, North Carolina, USA) and SPSS V.23.0 statistical package (SPSS, Chicago, Illinois, USA).
Results
AF hospitalisations, demographics and comorbidities
The characteristics of patients with AF who were hospitalised are presented in table 1. The proportion of patients with AF who were hospitalised in a given year compared with the total Korean patient population with AF in that year increased from 6.2% in 2006 to 9.1% in 2015. The proportion of females showed a modest increase, changing from 44.6% in 2006 to 46.4% in 2015 (P<0.001). The mean age increased from 69.5 (SE: 0.9) years in 2006 to 73.3 (SE: 0.5) years in 2015 (P<0.001). The proportion of elderly patients aged ≥70 years increased from 55.5% in 2006 to 69.5% in 2015 (P<0.001).
Characteristics of patients with AF hospitalisations
The most frequent coexisting conditions in hospitalised patients with AF were hypertension, heart failure and chronic obstructive pulmonary disease. Over the study period, the prevalence of several comorbid diseases increased significantly, with the largest increase of peripheral artery disease (2.0-fold; 12.9%–26.1%). Chronic kidney disease (CKD) also increased by 1.7-fold, from 10.8% in 2006 to 18.1% in 2015. CHA2DS2-VASc score and HAS-BLED score also significantly increased over the decade. The proportion of patients with intermediate and high economic status also increased significantly, while the proportion of low economic status decreased. The proportion of patients with AF initially diagnosed in primary care hospitals increased significantly, whereas the proportion of those diagnosed in secondary or tertiary referral hospitals decreased.
Trends of AF hospitalisations
From 2006 to 2015, the overall hospitalisation rate per 1 million Korean population increased significantly from 767 to 3986 per 1 million Koreans (relative increase, 420%; P<0.001; table 2). The significant increase of hospitalisation rate was observed across all age groups. The largest increase in hospitalisation rate was observed in the group aged ≥80 years (491%), followed by the group aged 70–79 years (267%). The relative rates of increase were higher in females than males (500% vs 350%; P<0.001). Therefore, the hospitalisation rate was higher in men from 2006 to 2009, but was higher in women since 2010. Hospitalisation due to major bleeding increased by 301%, from 241 to 966 per 1 million Koreans from 2006 to 2015 (P<0.001). Hospitalisation due to ischaemic stroke, AF control, MI and heart failure also increased by 116%, 294%, 94% and 146%, respectively (all P<0.001).
Trends of AF hospitalisation per 1 million Korean population between 2006 and 2015
The overall hospitalisation rate per 100 patients with AF also increased significantly from 13.4 in 2006 to 28.6 in 2015 (relative increase 113%; P<0.001). The increasing trend was consistent across all subgroups according to economic status and CHA2DS2-VASc score (all P<0.001, online supplementary table 3). Mean hospitalisations per 100 patients with AF with high CHA2DS2-VASc score (≥2) were consistently higher than those with CHA2DS2-VASc score from 0 to 1. Figure 1 shows the temporal trends of AF hospitalisations per 100 patients with AF according to main hospitalisation cause. The hospitalisations per 100 patients with AF mainly due to major bleeding, AF control, heart failure and SSS or PM related increased by 64%, 61%, 1% and 8%, respectively (all P<0.001). The magnitude of the increase in hospitalisation rates per 100 patients with AF was highest with RFCA for AF (110%; P<0.001). However, hospitalisations mainly due to ischaemic stroke (−12%; P<0.001) and MI (−21%; P<0.001) per 100 patients with AF decreased.

Temporal trends of AF hospitalisation per 100 patients with AF according to main hospitalisation causes between 2006 and 2015. *P value for increase trends <0.001. †P value for decrease trends <0.001. AF, atrial fibrillation; MI, myocardial infarction; PM, pacemaker; RFCA, radiofrequency catheter ablation; SSS, sick sinus syndrome.
Trends of AF hospitalisation costs
Table 3 shows temporal trends of AF hospitalisation costs. After adjusting for inflation, the overall cost of AF hospitalisations increased exponentially from €68.4 million in 2006 to €388.4 million in 2015 (relative increase, 468%; P<0.001). Across all subgroups according to age, sex, economic status and CHA2DS2-VASc score, the inpatient costs increased significantly (all P<0.001).
The total inpatient costs mainly due to major bleeding increased from €37.1 million in 2006 to €123.6 million in 2015 (relative increase, 233%; P<0.001). Total inpatient costs mainly due to ischaemic stroke, AF control and MI also increased by 168%, 468% and 71%, respectively (all P<0.001).
Trends of AF hospitalisation cost between 2006 and 2015
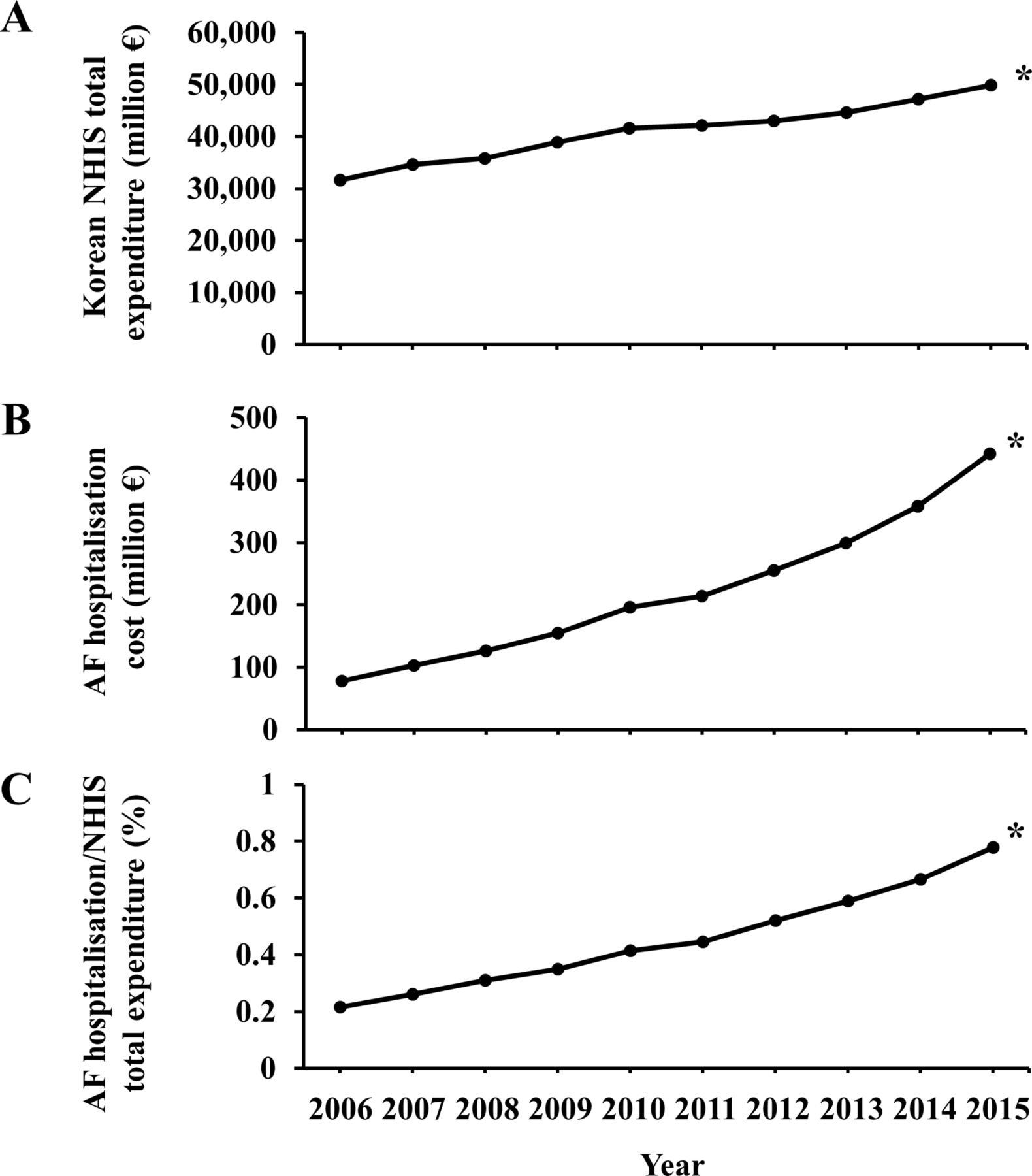
Over the same period, the annual Korean NHIS total expenditure increased by 58% from €31 589 million to €49 898 million.19 The proportion of AF hospitalisation cost to Korean NHIS total expenditure increased from 0.22% in 2006 to 0.78% in 2015 (figure 2, online supplementary table 4).
{kind=link}
{kind=link}
Temporal trends of medical cost between 2006 and 2015. (A) Korean NHIS total expenditure (million €), (B) total AF hospitalisation cost (million €) and (C) the proportion of total AF hospitalisation cost to Korean NHIS total expenditure (%). *P value for trends <0.001. AF, atrial fibrillation; NHIS, National Health Insurance Service.
Mean cost per hospitalisation for overall AF hospitalisation decreased by 3% from €2407 to €2337 (P<0.001). Mean cost per hospitalisation mainly due to ischaemic stroke, AF control, heart failure and RFCA for AF increased over the decade; however, mean cost per hospitalisation due to major bleeding and MI decreased over this period (table 4).
Mean cost per hospitalisation
Trends of AF treatment patterns
Table 5 shows the trends in AF treatment patterns. The use of oral anticoagulants significantly increased by 36% (from 26.8% to 36.4%; P<0.001), with increasing trends in both warfarin and non-vitamin K-dependent oral anticoagulant use. The use of P2Y12 inhibitors and statins increased by 165% and 160%, respectively, whereas aspirin use decreased by 19% (all P<0.001). Usage of digoxin decreased by 49%, while that of class Ic anti-arrhythmic drugs increased by 80% (both P<0.001).
Trends of AF treatment patterns between 2006 and 2015
In-hospital mortality and length of stay
Table 6 shows the trends of in-hospital mortality following AF hospitalisation. Overall in-hospital mortality significantly decreased from 7.5% in 2006 to 4.3% in 2015 (relative decrease 42%, P<0.001). The in-hospital mortality was highest in patients aged ≥80 years (7.7%) and in those with CKD (7.4%) and major bleeding (7.3%).
While mean lengths of hospital stay mainly due to major bleeding, ischaemic stroke, AF control, SSS or PM related and RFCA for AF decreased, those due to heart failure and MI increased over the time period from 2006 to 2015 (see online supplementary table 5).
In-hospital mortality for AF hospitalisation
Discussion
The main findings of our analysis of AF hospitalisation over a 10-year period in Korea are as follows: (1) AF hospitalisations have increased significantly for the last decade; (2) the majority of admissions occurred in elderly patients aged ≥70 years, and those aged ≥80 years demonstrated the largest increase of admissions and the greatest in-hospital mortality among all age groups; (3) the total costs of AF care were increased even after adjusting for inflation, with the proportion of AF hospitalisation costs to Korean NHIS total expenditure increasing to 0.78% in 2015 and (4) mortality associated with AF hospitalisations decreased significantly.
Increased AF hospitalisation
Our finding of increased AF hospitalisation rates is consistent with other nationwide studies.20 21 The increase of AF hospitalisation might be attributable to ageing of the general population and the increasing prevalence of risk factors including hypertension, diabetes mellitus and obesity.12 17 Almost 80% of hospitalised patients were ≥70 years of age, consistent with previous studies.3 21 Patients aged ≥80 years had the largest hospitalisation rate for any age group throughout the 10-year period, and had an exponential increase from 8185 in 2006 to 48 388 per 1 million people per year in 2015. Moreover, the in-hospital mortality in this age group was highest among all age groups. It is expected that the number of elderly Koreans aged ≥75 years will increase from 2.05 million in 2010 to 5.08 million in 2030, and to 11.0 million in 2060.22 Increasing AF hospitalisations with high mortality in this elderly group will give rise to an increased public healthcare burden and associated healthcare costs.
Since 2010, women had higher AF hospitalisation rates than men, with a higher rate of increase during 10 years. This sex difference is similar to that reported in previous studies in the USA and Scotland,21 23 and might be explained by a higher symptom burden and stroke risk in women with AF.24
Hospitalisation costs
In this study, total hospital costs per year increased exponentially by 468% over a 10-year follow-up. The annual Korean NHIS total expenditure increased by only 58%, while the proportion of AF hospitalisation cost to Korean NHIS total expenditure increased to 0.78% in 2015. Consistent with our findings, many previous studies have shown that the number of AF-related hospital costs have increased with ageing of the population and more prevalent risk factors such as hypertension and diabetes.20 21 Moreover, the number of RFCA shows a consistent increase over the past decade, which could contribute to the rise of hospital costs.
The mean length of hospital stays due to various causes, except heart failure and MI, decreased from 2006 to 2015 and mean cost per hospitalisation showed a slight decrease of −3% for the same period (perhaps related to the strong regulation of medication price and medical practice by the strict reimbursement system of Korea); however, the total cost increased significantly over the 10-year period. Increasing number of hospitalisations, ageing and increasing patients’ comorbidities and complexities are some drivers of these increasing costs, causing a major economic problem on the healthcare system.
Compared with some other countries,21 the mean length of hospital stay in Korea was significantly longer. This might be related to cheaper hospitalisation costs and generous reimbursement policies in Korea. Therefore, we should focus on limiting hospitalisations and on shortening the lengths of hospital stay. There are some potential means to reduce the cost of AF care, such as emergency department observation unit for acute onset AF, rhythm versus rate control and low molecular weight heparin use in patients hospitalised for AF.25–27
Treatment pattern and in-hospital mortality
Previous studies have reported that global burden of AF has increased exponentially.21 28 However, patients with AF showed a modest decrease in in-hospital mortality over the 10-year study period in our study. The rising prevalence and longer survival after onset of AF might be attributable, in part, to early disease detection due to improvements in surveillance methods and general medical care.
Along with decreased in-hospital mortality, we showed declines over time in stroke and MI admissions occurring in patients with AF. Our findings are in line with data that show a decline in stroke rates, including thromboembolic strokes, during the past few decades.29 In contrast, the number of hospitalisations mainly due to major bleeding among patients with AF increased over a 10-year period. These dual findings of decreasing stroke and MI and increasing bleeding admissions seemed to coincide with increased use of oral anticoagulants and P2Y12 inhibitors along with decreased use of aspirin. The switching of antithrombotic therapy from aspirin to oral anticoagulant as well as the increased use of P2Y12 inhibitors might help explain the decreased stroke and MI admissions and increased bleeding admissions.
Limitations
The present study has several limitations. Such studies using administrative databases might be susceptible to errors from coding inaccuracies. To minimise this problem, we examined the nationwide cohort and applied the definition that we already validated in previous studies that used a Korean NHIS sample cohort.13 15–17 Since we defined AF cases only with ICD-10 codes, it is possible that either paroxysmal or asymptomatic AF cases, which were not ascertained by these codes, were not recorded. Also, we could not analyse paroxysmal, persistent and permanent AF subgroups separately. We could not distinguish index admissions from re-admissions in the NHIS database, potentially leading to an overestimation of the number of hospitalisations. This study examines only in-hospital mortality without follow-up outcomes. However, this study analysed longitudinal data from the entire adult Korean population, using the largest nationwide Asian database available in the literature. Therefore, our findings should reflect the ‘real-world’ AF burden on a nationwide scale.
Conclusions
Hospitalisation rates for AF among Korean adults increased exponentially from 2006 to 2015, in association with an increase in comorbid chronic diseases. Mortality associated with AF hospitalisations decreased during the last decade, but hospitalisation costs have markedly increased. Prevention of AF hospitalisations and streamlined integrated AF management should be pursued in a holistic manner to lessen the healthcare burden of AF.30
Key questions
What is already known on this subject?
The healthcare burden of atrial fibrillation (AF) is growing considerably, and is mainly related to hospitalisations. However, the impact of AF on hospitalisations and mortality, and the economic burden of AF is less understood in Asian populations.
What might this study add?
AF hospitalisations have increased exponentially among Korean adults from 2006 to 2015, in association with an increase in comorbid chronic diseases. Mortality associated with AF hospitalisations decreased during the last decade, but hospitalisation costs have markedly increased.
How might this impact on clinical practice?
Prevention of AF hospitalisations and streamlined integrated AF management should be pursued in a holistic manner to lessen the healthcare burden of AF.
References
Footnotes
BJ and GYHL are joint senior authors.
DK and P-SY contributed equally.
Contributors BJ and GYHL contributed to the conception and design of the work and critical revision of the manuscript. DK contributed to the conception and design of the work, interpretation of data for the work and drafting of the manuscript. P-SY and EJ contributed to the acquisition and analysis of data for the work. HTY, T-HK, J-SU, JYK, H-NP and M-HL contributed to the conception and design of the work and revising the manuscript. All authors approved the final version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was supported by a research grant from the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (NRF-2017R1A2B3003303), and grants from the Korean Healthcare Technology R&D project funded by the Ministry of Health & Welfare (HI16C0058, HI15C1200).
Competing interests GYHL: consultant for Bayer/Janssen, BMS/Pfizer, Biotronik, Medtronic, Boehringer Ingelheim, Novartis, Verseon and Daiichi-Sankyo. Speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim and Daiichi-Sankyo. No fees are directly received personally.
Patient consent Not required.
Ethics approval This study was approved by the Institutional Review Board of Yonsei University Health System (4-2016-0179).
Provenance and peer review Not commissioned; externally peer reviewed.