Article Text

Abstract
Background Epidemiological studies have suggested that female hormones might play a role in asthma and that menopausal hormone therapy (MHT or hormone replacement therapy (HRT)) might increase the risk of asthma in postmenopausal women. The only prospective study addressing this issue reports an increase in the risk of developing asthma which was similar for oestrogen alone and oestrogen/progestagen treatment.
Methods The association between the use of different types of MHT and the risk of asthma onset in postmenopausal women was investigated prospectively from 1990 to 2002 by biennial questionnaires as part of the French E3N cohort study. Asthma onset was considered to be the time of medical diagnosis of asthma cases occurring during the follow-up of women who were asthma free at baseline. Cox proportional hazards models were used, adjusting for potential confounding factors.
Results Among 57 664 women free of asthma at menopause, 569 incident cases of asthma were identified during 495 448 years of follow-up. MHT was related to an increased risk of asthma onset (HR=1.20, 95% CI 0.98 to 1.46) among recent users. The increase in risk of asthma onset was only significant among women reporting the use of oestrogen alone (HR=1.54, 95% CI 1.13 to 2.09) particularly in never smokers (HR=1.80, 95% CI 1.15 to 2.80) and women reporting allergic disease prior to asthma onset (HR=1.86, 95% CI 1.18 to 2.93). A small increase in the risk of asthma onset associated with the use of oestrogen/progestagen was also observed in these subgroups.
Conclusion Postmenopausal use of oestrogen alone was associated with an increased rate of newly diagnosed asthma in menopausal women.
- Asthma
- epidemiology
- menopausal hormone therapy (MHT)
- hormone replacement therapy (HRT)
- asthma epidemiology
- macrophage biology
Statistics from Altmetric.com
- Asthma
- epidemiology
- menopausal hormone therapy (MHT)
- hormone replacement therapy (HRT)
- asthma epidemiology
- macrophage biology
Introduction
The major increase in asthma prevalence observed in most developed countries in recent years1 suggests that it may in part be due to environmental factors. Differences in asthma incidence during the life cycle suggest that reproductive hormones influence the development of asthma and asthma severity.2 Asthma is more frequent in girls after menarche than before.3 Adult asthma and hospital admissions for asthma are more prevalent in women than in men, and asthma severity has been shown to vary during the menstrual cycle and pregnancy.4 In addition, the incidence of asthma tends to decrease after the menopause.5 The increase of asthma onset in postmenopausal women with increasing weight points to an endocrine mechanism such as increased endogenous oestrogen synthesis.6 Menopausal hormone therapy (MHT) might therefore play a role in asthma onset.
Different studies have investigated the role of MHT in asthma. Cross-sectional studies have reported an association between prevalent asthma and asthma-like symptoms and MHT use in perimenopausal7 and postmenopausal women,8 9 with a larger effect in lean women. However, these studies were cross-sectional and therefore could not evaluate the effect of MHT on asthma onset. None of these studies evaluated the risk related to different types of MHT. To date only one cohort study, the Nurses' Health Study (NHS), has suggested that MHT use is associated with an increased risk of developing asthma. It observed a similar significant (twofold) increase in risk with the use of oestrogen alone or oestrogen plus progestin.2
The mechanisms underlying the link between hormonal factors and asthma risk are still not clearly understood.10 Knowing whether MHT affects this risk and, if so, whether different preparations have a similar effect would provide a useful insight into the mechanisms by which the hormonal milieu acts on the airways.
We used data from the E3N study, a large cohort of French women followed for >10 years, to evaluate the association between asthma onset and MHT use with special focus on the types of MHT and the duration of use.
Methods
Study population: the E3N cohort
E3N, a prospective cohort initiated in 1990, consists of 98 995 French women born between 1925 and 1950 and insured under a health insurance plan covering mostly teachers. The study was approved by the French National Commission for Data Protection and Privacy. E3N is the French component of the European Prospective Investigation into Cancer and Nutrition (EPIC). Participants, who gave written informed consent, completed biennial self-administered questionnaires addressing medical history, menopausal status, and a variety of lifestyle characteristics.
Definition of incident cases of asthma
Women were considered incident cases of asthma if they stated at baseline (menopause) that they had never had an asthma attack and met the American Thoracic Society (ATS) criteria for asthma definition at follow-up (“Have you ever had asthma attacks?” and, if yes, “Was this diagnosis confirmed by a doctor?”),11 with a coherent reported age of asthma onset (time of first attack between baseline and 2002).
Identification of MHT use
Information on lifetime use of hormonal treatments was first recorded in the 1992 questionnaire. For each episode of treatment (defined as the non-stop use of the same hormonal brand or combination), brand name, age at initiation of use and duration were recorded. The information was updated in each of the subsequent questionnaires. The complete history of MHT use was established using data from all the questionnaires. MHT use was categorised by (1) type of oestrogen: weak oestrogens (orally or vaginally administered promestriene or estriol) or oestradiol compounds (unopposed MHT consisted almost exclusively of oestradiol compounds; only 1.3% of women ever used conjugated equine estrogens (CEEs) corresponding to 8% of the total person-years of follow-up) and (2) type of oral progestagen used in association with the oestrogen: none, micronised progesterone, pregnane or norpregnane derivatives, and testosterone derivatives.
Body mass index
Body mass index (BMI) was calculated from the height and weight self-reported in each questionnaire. BMI was used in the different analyses as a continuous or categorical time-dependent variable. Information on anthropometric measurements provided by our questionnaire has been shown to be highly reliable.12
Other information
Information on tobacco smoking was reported in each questionnaire and respondents were categorised as never, past, regular or occasional smokers. The last two categories were combined into a “current smokers” category. Atopy was defined as present if the woman reported diagnosis of allergic rhinitis, eczema or any other allergic disease on the questionnaire prior to asthma onset.
Population for analysis and follow-up
Our analysis was based on 57 664 postmenopausal women, corresponding to 495 448 person-years of follow-up. These women were free of asthma at inclusion, and all subsequent self-reports of asthma onset were validated according to the ATS criteria. Subjects contributed person-time until the date of the first asthma attack or July 2002 (date of dispatch of the seventh questionnaire), whichever occurred first.
Figure 1 presents a diagram of the initial population, the reasons for exclusion and the population included in the analysis.

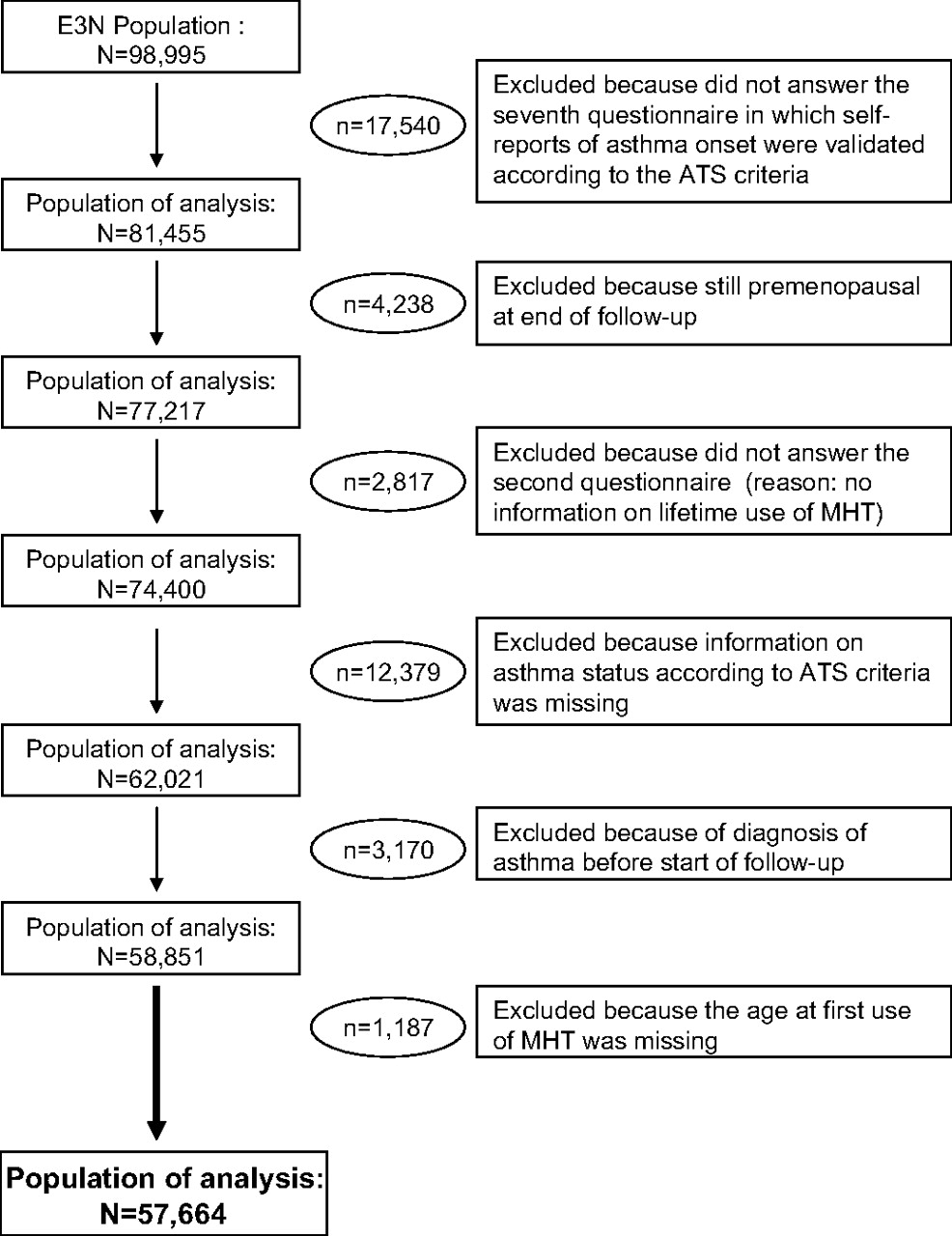{kind=link}
Diagram of the initial population, the reasons for exclusion and the population included in the analysis. ATS, American Thoracic Society; MHT, menopausal hormone therapy.
Statistical analysis
HRs for asthma were estimated using Cox proportional hazards models, with age as the time scale. We adjusted our model for tobacco smoking and BMI included in the model as time-dependent (or time-varying) covariables, and for other risk factors. MHT use was included in the model as a time-dependent variable. A woman contributes to person-years of ever use from the date she starts her treatment to the end of the follow-up, contributes to person-years of recent use from the date she starts her treatment to 1.5 years after she stops and contributes to person-years of past user thereafter. This cut-off (1.5 years) was chosen because 65% of the cases occurring after cessation of MHT use did so within a year and a half of cessation. The reference group in each model consisted of women who indicated that they had not yet used any MHT. Further analyses were conducted after stratification of the data by hysterectomy, type of menopause (surgical or non-surgical), smoking status as well as the atopic status of the women. All tests of statistical significance were two sided, and significance was set at the 0.05 level. All analyses were performed using SAS software, version 9.1 (SAS Institute., Cary, North Carolina, USA) (for further details of methods used, see the online supplement).
Results
Among the 57 664 women who reported being postmenopausal and had information on MHT use, there were 569 incident cases of asthma between 1992 and 2002, corresponding to an incidence of 1.15/1000 per year.
Never user of MHT accounted for 35.7% of the person-years, past users for 4.5%, recent users for 55.8% and 4% did not provide information on duration of treatment. The mean age of ever users and never users at the start of follow-up was 52.25 years (SD=4.00) and 54.58 years (SD=4.74) (p<0.0001), respectively. Women excluded from the analysis were less likely to have used MHT or oral contraceptives, and were slightly older and had a larger BMI (χ2 test p<0.001) than those included.
Table 1 presents the characteristics of ever users and never users of MHT included in the analysis. After adjusting for age, ever users were more likely to have a lower BMI (p<0.001) and to have ever used oral contraceptives (p<0.0001) than never users.
Characteristics of the study population (n=57 664), E3N cohort study
Surgical menopause was reported by 10% of the women. The use of oestrogen alone was reported by 9.4% of the women with natural menopause and by 28.1% of the women with surgical menopause. Hysterectomy was reported by 19% of the women. Among women who had a hysterectomy, 58% reported a natural menopause and 27% a surgical menopause (n=2986); 36% of these reported using oestrogen alone (see online supplement).
The HR of asthma onset among women who had ever used MHT was 1.21 (95% CI 1.00 to 1.46) compared with never users after adjusting for age, smoking, BMI, oral contraceptive use, parity and total caloric intake (table 2).
Hormone therapy and asthma onset among postmenopausal women, E3N cohort study
Among recent MHT users the HR was 1.20 (95% CI 0.98 to 1.46), and was 1.16 (95% CI 0.86 to 1.57) among past users. Women who reported using MHT for <2 years had an HR of 1.25 (95% CI 1.02 to 1.53) and those who reported using MHT for ≥2 years an HR of 1.09 (95% CI 0.85 to 1.38), compared with never users (table 2).
Oestrogen alone was reported as the last treatment used by 11.2% of the women. These women were at higher risk of asthma onset (HR=1.54, 95% CI 1.13 to 2.09) compared with never users. The risk was not significantly increased among women who reported oestrogen/progesterone (18.3%), a combination of oestrogen and another progestagen (54.7%) or another MHT (15.8%) as the last treatment used. In subsequent analyses, users of any type of oestrogen/progestagen were therefore combined into an “oestrogen/progestagen users” category. The risk of asthma onset associated with the use of oestrogen alone was significantly different from that associated with the use of oestrogen/progestagen (test for homogeneity p=0.04). The route of oestrogen administration (oral or transdermal) did not significantly affect the risk (table 2).
For recent users of oestrogen alone the HR of asthma onset was 1.67 (95% CI 1.20 to 2.27), while for past users it was 1.04 (95% CI 0.51 to 2.12). Among women who reported using oestrogen alone for <2 years the HR was 1.60 (95% CI 1.12 to 2.27) while among those who reported using oestrogen alone for ≥2 years the HR was 1.39 (95% CI 0.84 to 2.31). These HRs were non-significantly different (test for homogeneity p=0.63). The route of administration of oestrogens without progestagen did not affect the risk. Among women reporting the use of oestrogen/progestagen there was no indication of an increase in the risk of asthma onset whatever the duration or recency of use or route of oestrogen administration (table 3).
Hormone therapy and asthma onset among postmenopausal women by type of treatment, E3N cohort study
Among never smokers, MHT use was significantly related to the risk of asthma onset (HR=1.45, 95% CI 1.10 to 1.90) while among smokers the HR was 1.02 (95% CI 0.79 to 1.31) (test for interaction p=0.09) (see online supplement table E1). Among women who reported using oestrogen alone, the HR was 1.80 (95% CI 1.15 to 2.80) for never smokers and 1.31 (95% CI 0.85 to 2.03) for ever smokers (test for interaction p=0.37). Never smokers using oestrogen/progestagen had an HR of 1.38 (95% CI 1.02 to 1.86), while no effect (HR=0.92, 95% CI 0.69 to 1.21) was observed in ever smokers (test for interaction p=0.16) (table 3).
Higher BMI was associated with an increased risk of asthma onset (p for trend <0.001) but there was no indication of an interaction between MHT use and BMI on the risk of asthma (p=0.45). Among women with a BMI <22 the HR of oestrogen alone users was 1.25 (95% CI 0.65 to 2.40), among women with a BMI from 22 to 25 the HR was 1.67 (95% CI 0.93 to 3.01) and among women with BMI >25 the HR was 1.54 (95% CI 0.99 to 2.39).
After stratification by the presence of hysterectomy or the type of menopause, we observed a small increased risk among non-hysterectomised women using oestrogen alone and among women declaring a natural menopause. However, the small number of cases in some of the subgroups limited the interpretation of the results (see online supplement tables E2 and E3).
Women who reported a diagnosis of allergic disease prior to asthma onset appeared to have a larger risk of asthma related to MHT than their counterparts. An increased risk of asthma was present for the use of oestrogen alone (HR=1.86, 95% CI 1.18 to 2.93) and a marginal significant increase was observed for the use of oestrogen/progestagens (HR=1.39, 95% CI 1.01 to 1.91) in women with allergic disease as compared with women without allergic disease (table 4).
Hormone therapy and asthma onset among postmenopausal women by atopic status, E3N cohort study
Discussion
In this large prospective study of French women including 569 incident cases of asthma over 495 448 person-years, use of oestrogen alone as last treatment was significantly associated with an increased risk of asthma onset in postmenopausal women, after adjustment for potential confounding factors. The increase in risk was mostly observed among women reporting an allergic disease prior to asthma onset and in never smokers. In these subgroups, the risk of asthma onset was strongly related to the use of oestrogen alone and a marginal association was observed with the use of oestrogen/progestagens.
Our results agree in part with other recent reports. In the NHS, MHT use was significantly related to the risk of asthma onset in postmenopausal women. However, a similar increased risk was reported for both oestrogen alone and oestrogen/synthetic progestin. The effect was stronger in current users, and the risk diminished with time after cessation. In addition, an interaction was observed between MHT and BMI, with a larger risk of newly diagnosed asthma in lean women.2
In the cross-sectional Copenhagen City Heart Study, the prevalence of self-reported asthma was significantly related to MHT in non-smokers.9 Two further recent cross-sectional studies reported an association between prevalent asthma and asthma-like symptoms with MHT use in women aged 46–547 and postmenopausal women,8 but only in lean women. None of these cross-sectional studies provided information on the type of hormone replacement therapy (HRT) used.
In our study, the increased risk of asthma onset among women using MHT was present only in users of oestrogen alone. The effect was observed only in recent users including current users and women for whom time since last use was <1.5 years. Overall no increased risk was observed in users of oestrogen/progestagen, while a marginally significant increase was observed among women reporting a diagnostic of allergic disease prior to asthma onset and among non-smokers.
Our study and the NHS are comparable in design, number of cases and person-years of follow-up. Results of both studies agree on the adverse effect of oestrogen-alone MHT; however, we observed conflicting results with regards to oestrogen/progesterone MHT in the overall analysis. The marginal increased risk observed in some subgroups of our population is difficult to compare given that no stratified data on smoking or allergic disease are presented in the report from the NHS.2
Several mechanisms have been proposed to explain the role of female hormones in asthma risk. However, there is still some uncertainty. Oestrogen appears to have both anti-inflammatory and proinflammatory effects, depending on criteria such as cell types, conditions in the milieu, oestrogen concentration and the target organ.13 While oestrogen may have a proinflammatory effect regulating the response to allergens, it may also downregulate the traffic of eosinophils to the lung during the effect or phase of the response to antigens.14 It has also been shown that oestrogen acts to downregulate airway hyper-responsiveness in a dose-dependent manner and in a relatively rapid, non-genomic manner by enhancing the activity of endothelial nitric oxide synthase.15 Several animal studies have reported increased susceptibility to allergic airway disease in female mice compared with male mice. Oestrogens appear to exert most of their effects through oestrogen receptors α and β, both of which are present in the lung.10 Ovariectomised rats developed less airway inflammation than controls, and oestrogen replacement re-established airway inflammation to the level found in intact females. A recent study suggested that female rats have fewer T regulatory (Treg) cells and therefore less protection against inflammatory stimuli such as allergens.16 Oestrogen (oestradiol) has also been shown to alter β2-adrenergic responsiveness17 and to activate endothelial nitrite oxide synthase,18 involved in the pathogenesis of asthma. Oestrogen is capable of inhibiting the activity of 11-β-hydroxysteroid dehydrogenase type I isoenzyme, thereby reducing its ability to regenerate active cortisol from cortisone, and cortisol is an extremely powerful anti-inflammatory agent that may be protective against the development of chronic inflammation.19 Finally, oestrogen levels have been related to lower levels of adiponectin, a protein that is secreted exclusively by adipocytes, acts as an insulin sensitiser and has anti-inflammatory properties.20 This cytokine is inversely associated with fat mass and insulin resistance, and has been proposed as a link between obesity and inflammation in humans.21 Most probably several of these mechanisms and pathways play a role and interact with individual susceptibility.
Unopposed oestrogens are used in women who have had a hysterectomy, and hysterectomy may lead to hormonal changes and respiratory morbidity, or alternatively a common underlying pathology may lead both to gynaecological morbidity resulting in hysterectomy and to asthma.8 In our data, among MHT never users, the HR of asthma onset associated with hysterectomy was 1.31 (95% CI 0.85 to 2.01), suggesting that hysterectomy could not fully explain the increased risk observed among the oestrogen users. Only 38.8% of women with hysterectomy reported using oestrogen alone and the reason for hysterectomy was unknown. In stratified analyses by hysterectomy or type of menopause, there was no indication of differential effects of MHT in these subgroups.
We did not observe a clear increase in the risk of asthma onset with oestrogen/progestagen treatment in contrast to the results of the NHS. In our population, a marginal increased risk was restricted to never smokers and women who reported a diagnosis of allergic disease prior to asthma onset . While we do not have a clear explanation for this, a combined hormone regimen has been shown to affect the lung functions of postmenopausal women positively while oestrogen alone has no effect.22 Progesterone has receptors in the lungs and trachea, and can therefore have local effects at these sites and cause ventilatory stimulation via chemoreceptor activity.23 In a rat model of allergic lung inflammation, oestradiol increased the number of neutrophils, eosinophils and mononuclear cells in the bronchoalveolar lavage of ovariectomised allergic rats, whereas progesterone induced an additional reduction. Degranulation of bronchial mast cells from ovariectomised rats was reduced after in vitro challenge, an effect reversed by oestradiol but not by progesterone.24 These authors suggest that intensity of allergic lung inflammation might be related to the oestradiol to progesterone ratio at the time of immune sensitisation and antigen challenge. Exogenous progesterone might also downregulate β2-adrenoceptors, which would explain part of the difference between MHTs.17 A possible explanation for the difference of effect observed between the NHS and our study could be the difference in the type of progestorene used by US and French women and/or the ratio of oestrogen to progesterone. In the USA, combined MHT uses mostly medroxyprogesterone acetate (MPA) while in our study this type of treatment represented only 10.2% of person-years of follow-up. Micronised progesterone corresponded to 19.7% and other pregnane and norpregnane derivatives to 38.3%.
The association of MHT use with increased risk of asthma onset was more apparent among never smokers, as reported in other studies.7 9 This might be due to the antioestrogenic effect of smoking25 or to the difficulty of isolating the additional effect of MHT among smokers. In contrast to other studies, we did not observe an interaction between BMI and MHT use.2 7 8 An earlier analysis of our data found a significant association between BMI and the risk of asthma onset in both MHT ever users and never users.6 The lack of interaction in our data might be due to the BMI distribution of our population, which was leaner than that of the NHS.
Women reporting a diagnosis of allergic disease prior to asthma onset had a higher risk of MHT-related asthma than their counterparts. A cross-sectional study among English women by Jarvis et al8 reported that current use of HRT was related to wheeze but not related to markers of allergy (immunoglobulin E). No data on atopic asthma were presented. Our data suggest that women with an allergic predisposition might be more susceptible to the effect of MHT in developing asthma. However, these results should be interpreted with caution given the small number of cases in some subgroups and the potential misclassification of allergic disease based only on women's reports at baseline and in the follow-up questionnaires.
The strengths of our study include the large number of postmenopausal incident cases of asthma. While we imputed age at menopause for some women with missing information (n=9585), the results remained similar when these women were excluded from the analysis. Information on current and past MHT use was updated every 2 years, decreasing the potential risk of misclassification of MHT. In our analysis, we used the information relating to the hormone therapy at the time of asthma onset. Fifty-eight percent of women reporting the use of oestrogen alone at the time of asthma onset or as last treatment before asthma onset had previously used another MHT. This supports our finding that the increased risk of asthma onset is linked to oestrogen use. We also conducted additional analyses in which exposure was defined as exposure to the MHT with the longest duration of use. Results remained similar. For 80.5% of the women, the last treatment used was also the longest. In addition, most participants in the E3N cohort were teachers, with a high level of education and health consciousness,26 while the prospective design and high rate of follow-up of our study (3.8% lost to follow-up) minimised the possibility of recall bias or bias due to loss of follow-up.
Our definition of asthma met the ATS criteria, and there was a consistent reported date of asthma onset (time of first attack between 1990 and 2002). In addition, we conducted an analysis including as asthma cases only women who reported having asthma in at least two questionnaires (persistent asthma). Results were similar to those observed when all cases of asthma onset were included. Some women may suffer not from asthma but from chronic obstructive pulmonary disease (COPD). We did not measure pulmonary function so the possibility of COPD in older women, particularly ex- and current smokers, cannot be excluded. However, 51% of the cases were non-smokers and were therefore unlikely to have COPD. Furthermore, asthma risk was related to MHT use in non-smokers, suggesting that neither smoking nor the misclassification of asthma as COPD could explain the association observed between MHT and asthma incidence. In the NHS, MHT was not related to newly diagnosed COPD.2
Our results could be biased if MHT users systematically reported more asthma attacks or if asthma was diagnosed more often in MHT users because of more frequent visits to the doctor. During the follow-up, 93% of the MHT users had a mammogram versus 78% of the non-users. However, our population had access to free medical care and there is no reason to believe that MHT users make more frequent medical visits than non-users for non-gynaecological-related health issues.
In conclusion, our study shows an association between the use of oestrogen alone as MHT and asthma onset in a large cohort of postmenopausal women. This effect might be linked to an increase in airway inflammation mediated by different pathways, such as inflammatory cytokine release or stimulation of nitric oxide synthesis. The increase in asthma risk associated with MHT must be judged in the light of all other health effects of MHT use, including its beneficial effect on the quality of life of menopausal women.
Acknowledgments
The authors are indebted to all participants for providing data and to practitioners for providing pathology reports. The authors are grateful to R Chaït, M Fangon, M Niravong and L Hoang for managing the data.
References
Footnotes
Linked articls 129205.
Funding Mutuelle Générale de l'Education Nationale, the Institut de Cancérologie Gustave Roussy and the Institut National de la Santé et de la Recherche Médicale. IR was supported by the National Center for Environmental Health-Centers for Disease Control and Prevention, Atlanta, Georgia, USA. AF was supported by the Cancéropôle Région Ile de France. BL was supported by the GA2LEN project (EU contract FOODCT-2004-506378).
Competing interests None.
Ethics approval The study was approved by the French National Commission for Data Protection and Privacy.
Provenance and peer review Not commissioned; externally peer reviewed.