Recent developments in obstetrics
BMJ 2003; 327 doi: https://doi.org/10.1136/bmj.327.7415.604 (Published 11 September 2003) Cite this as: BMJ 2003;327:604
- Andrew H Shennan, professor of obstetrics1
Introduction
Two of the most challenging areas in antenatal care are prematurity and pre-eclampsia. Between them they affect one in 10 of all pregnant women, and their prevalence is static. Until recently management options have been limited. Improved understanding of the basic pathophysiology is changing this.
Sources and selection
This article describes those advances that have made an impact on the management of prematurity and pre-eclampsia. Another major concern in obstetrics is the rising number of interventions, particularly caesarean sections, without obvious benefit to mother or baby. Recent research has highlighted several simple but effective strategies that could help influence this trend. These include management of previous caesarean sections and breech presentation and more appropriate use of fetal monitoring and epidurals in labour; knowledge of these will be valuable to any clinician who comes into contact with pregnant women. The articles selected are from relevant searches in English from Pubmed and the Cochrane Collaboration, as well as the author's own experience through research and reviewing.
Pre-eclampsia
The current structure of antenatal care developed around detecting pre-eclampsia. The detection of hypertension and proteinuria, the defining signs of this syndrome, is the key aim of frequent surveillance in pregnancy. Pre-eclampsia occurs in about 3% of pregnant women and results in around 100 000 maternal deaths per year worldwide. The fetus is also affected, directly through placental insufficiency and indirectly through iatrogenic delivery; this accounts for 25% of all infants with a very low birth weight (< 1500 g). The onset and course of pre-eclampsia are unpredictable, and it therefore results in enormous use of health resources. Accurate prediction and targeted preventive measures would have enormous benefit.
Prediction
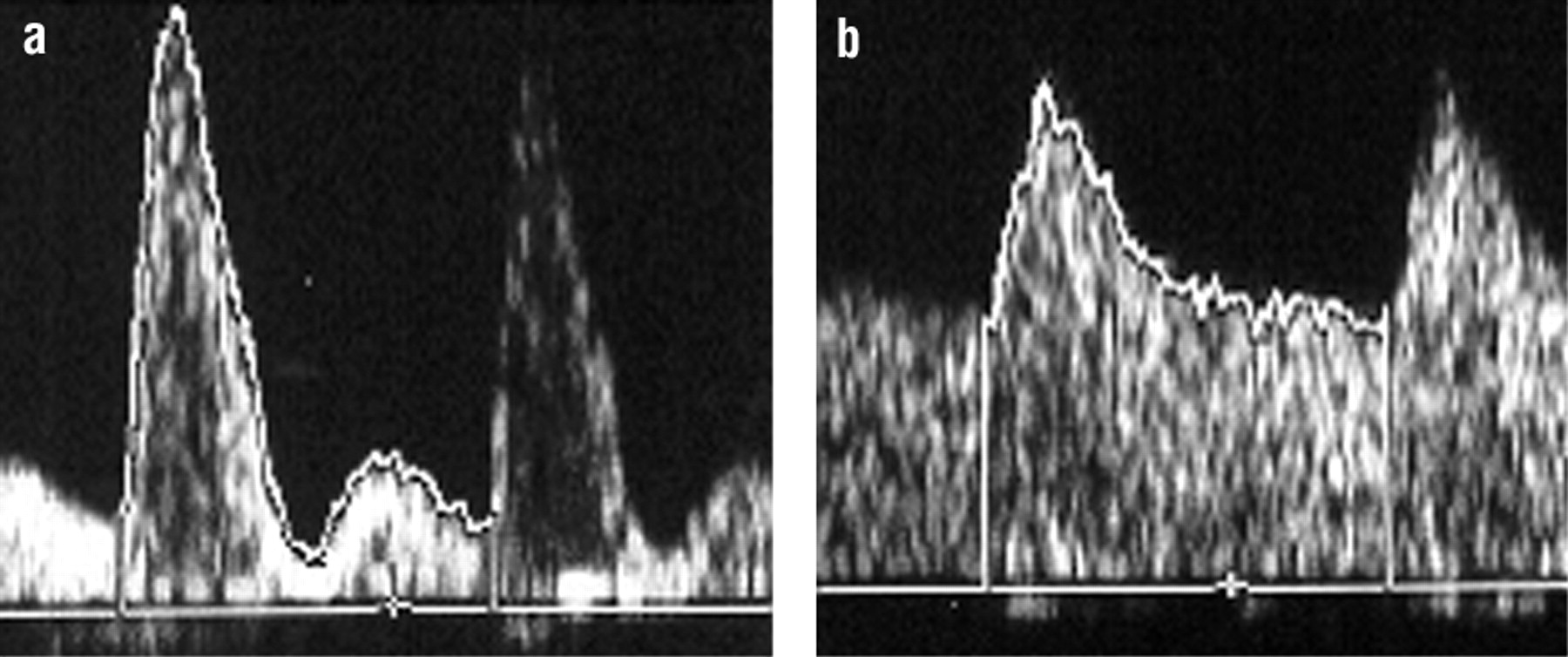
Many biochemical substances, principally of placental and endothelial origin, increase in pre-eclampsia. However, their predictive value to detect susceptible women before clinical presentation is poor. As the disorder originates in the placenta, blood flow in the uterine artery is abnormal in most women destined to present with the syndrome. A population at risk can be targeted for intervention (fig 1) by using Doppler ultrasound to measure blood flow in the uterine artery in the second trimester. This biophysical test is currently the best predictor of pre-eclampsia. Positive predictive values are similar in both high and low risk groups, so 20% of women with an abnormal Doppler result will develop pre-eclampsia.1 2

Flow velocity waveforms in the uterine artery as shown by Doppler analysis. a: abnormal flow velocity waveforms—high resistance index, early diastolic match. b: normal flow velocity waveforms—low resistance index, no match
{kind=link}
Recent developments
Pre-eclampsia affects around 3% of pregnant women and accounts for 25% of all babies with a very low birth weight (< 1500 g). Doppler ultrasound of theuterine artery can identify women at risk
Low dose aspirin (75 mg) given prophylactically will reduce the chance of developing pre-eclampsia by 15%, with a similar reduction in fetal death. This should be considered in women at risk
The second trimester use of vaginal ultrasound to measure cervical length and the detection of vaginal fetal fibronectin are better predictors of preterm delivery than previous history
Although infection has a key role in the aetiology of early preterm delivery, evidence regarding the use of prophylactic antibiotics is contradictory since benefit may be related to the choice, route, and timing of treatment
There is no evidence that asymptomatic women with abnormal vaginal flora benefit from antimicrobials
Women with a breech presentation at term who plan a vaginal delivery have a 3% increased risk of death or serious morbidity to their baby. External cephalic versionshould therefore be offered
Intrapartum intervention can be reduced by avoiding unnecessary electronic fetal monitoring, encouraging vaginal delivery with previous caesarean section, and using low dose epidurals
Prevention
Aspirin at low dosage has been evaluated extensively as an agent to prevent pre-eclampsia, with a sound rationale of reversing the imbalance of prostacyclin and thromboxane that is found in women with the disease. In 32 randomised controlled trials including nearly 30 000 women, low dose aspirin results in a 15% decrease in pre-eclampsia, with a similar reduction in the chance of fetal death.3 4 Babies are also less likely to be delivered prematurely, and the benefit is independent of risk status. Few interventions in perinatal medicine actually reduce the risk of the baby dying. Targeting women with an abnormal Doppler ultrasound can reduce the number needed to treat (NNT) considerably. Figure 2 shows how the positive predictive value of a test and the reduction in relative risk of an intervention will influence the number needed to treat. Even with a positive predictive value of around 20% (as found with uterine Doppler ultrasound) and a relative risk reduction of 15%, the number needed to treat can still be reduced substantively and make clinical application worth while. The value of screening women at low risk has, however, not been established.

Influence of positive predictive value and relative risk reduction (RRR) on the numberneeded to treat (NNT)
{kind=link}
The benefit of the intervention may also be better in women identified by abnormal Doppler results. In five randomised controlled trials including women treated with aspirin after abnormal uterine Doppler ultrasounds, the reduction of relative risk in preeclampsia was nearer 45%.5 Recently antioxidants in the form of high dosages of vitamins C (1000 mg) and E (400 IU) have also been used successfully in reducing pre-eclampsia by more than 50%.6 Figure 2 also shows the numbers needed to treat when the intervention results in a relative risk reduction of 50%. Again the rationale for using these vitamins is scientifically sound as oxidative stress seems to be a key feature of the pathophysiology. This study was performed in women principally identified by abnormal Doppler ultrasounds and needs confirmation in other groups before widespread use of vitamins C and E can be recommended.6 However, the combination of predicting women at risk and targeting them with a safe intervention seems to be a sound strategy to limit the number needed to treat to prevent one case.
Management
The management of pre-eclampsia entails close surveillance and delivery. Otherwise it is empirical, aimed at reducing morbidity or mortality. It includes antihypertensive agents, which can be used to halve severe hypertension (relative risk reduction 0.52, confidence interval 0.41 to 0.64).7 This is likely to reduce the risk of cerebral haemorrhage, which occurs in half the women who die.8 Controlling blood pressure does not, however, alter progression of the disease.
The eclampsia trial showed that magnesium sulphate was the drug of choice to prevent further fits after eclampsia,9 but the value of prophylactic treatment with anticonvulsant drugs has been uncertain. As large numbers of women would need to be treated the benefits of prophylactic treatment are important to ascertain. The Magpie study compared giving magnesium sulphate with giving placebo to more than 10 000 women with pre-eclampsia.10 The chance of eclampsia was 0.8% if allocated magnesium sulphate compared with 1.9% in the controls; this represented 11 fewer fits per 1000 women treated. No benefit to the baby was found, although placental abruption may be less common in the group treated with magnesium sulphate. An eclamptic fit indicates serious underlying disease and is usually self limiting and not inherently life threatening, although undesirable. The importance of these findings will therefore depend on previous practice and the population treated. For example, in the United States where magnesium sulphate is used extensively in women at relatively low risk its use may now decline. However, women at high risk are likely to benefit as a trend has become obvious towards fewer maternal deaths in the Magpie study (relative risk 0.55, 95% confidence interval 0.26 to 1.14), and there are physiological reasons why magnesium sulphate might benefit other aspects of sequelae of pre-eclampsia.
Prematurity
Preterm delivery accounts for 65% of neonatal deaths and 50% of neurological disability in childhood. Spontaneous preterm labour or prelabour rupture of the membranes account for 80% of preterm deliveries. Prematurity rates have not changed in recent decades.
Prediction
A short cervix identified on vaginal ultrasound has a good predictive value for early delivery, even in a low risk group, and a cervical length of less than 15 mm will result in a 50% chance of delivery before 32 weeks' gestation.11 The predictive value in multiple pregnancies is similar.12 Identifying fetal fibronectin in vaginal secretions after 22 weeks' gestation also has a strong association with preterm delivery.13 Both these tests perform far better than previous history as predictors of preterm delivery, which has traditionally been the way to identify a group at risk, as most women with recurrent prematurity will achieve a term pregnancy in their subsequent pregnancy. Although it is impractical to screen all women, populations at risk could be targeted with these tests to identify groups for intervention.
Prevention
Few agents can stop uterine contractions effectively, and acute tocolysis has never been shown to reduce perinatal mortality. Delivery may be prevented in the short term, which will allow steroids to be given to the mother or enable transfer to a suitable neonatal unit. A new tocolytic, atosiban (an oxytocin antagonist), is no more effective than β agonists but has fewer side effects and is therefore likely to be safer.14 Treatment has therefore focused on prophylactic measures.
Cervical cerclage—Elective cervical cerclage has previously shown only marginal benefit in preventing preterm delivery, and attention is now focused on cerclage in women identified at risk from a short cervix. Preliminary results show that this may be beneficial, although they are based on very small numbers.15 Some retrospective evidence shows that transabdominal cerclage may have a role in cases where transvaginal cerclage has failed.16
Antibiotics—Although preterm labour is multifactorial, it is often associated with and caused by infection, particularly if very preterm. Both bacterial vaginosis and vaginal infection with group B streptococci increase the risk of preterm delivery. Unfortunately randomised controlled trials have shown that using metronidazole in women at low risk who are positive for bacterial vaginosis does not reduce this risk.17 Targeting women at risk has shown variable results, but some randomised controlled trials show that antibiotics can even increase the risk of preterm delivery.18 More recently oral clindamycin given early to women with abnormal vaginal flora has shown some value in reducing late miscarriage and preterm delivery.19 Therefore the timing, type, and population targeted may determine if treatment is beneficial. The ORACLE trial considered if antibiotics were valuable in preterm labour and prelabour rupture of the membranes.20 Erythromycin significantly reduced the chance of delivery within one week while improving neonatal outcome in women with prelabour rupture of the membranes.20 Importantly co-amoxiclav increased the risk of necrotising enterocolitis and is not recommended with prelabour rupture of the membranes. Asymptomatic bacteruria should be treated as the treatment reduces prematurity.
Tocolytic agents—Although acute tocolysis is of limited benefit, its use is generally restricted by unwanted side effects. Atosiban can be given for prolonged periods, and its use as a prophylactic agent is now being assessed. Calcium channel blockers such as nifedipine also have fewer side effects and are equally efficacious to atosiban, although they are unlicensed for use in pregnancy. Non-steroidal antiinflammatory drugs can cause renal and ductal problems in the fetus. Current studies are evaluating the cyclo-oxygenase-2 inhibitors, which theoretically may be as efficacious at preventing delivery while limiting these unwanted side effects, thus allowing their use as a prophylactic measure.
Other strategies—Progesterone, given either intramuscularly or by vaginal pessary to women at risk, has shown some benefit in reducing preterm delivery in at risk women, and confirmatory trials are eagerly awaited.21 22 Initial reports show that fish oils may reduce the incidence of preterm labour in women with a previous history, although the scientific rationale underpinning this has not been robustly tested.23 Confirmation is required in prospective trials. In the mean time the biggest impact to prevent prematurity is probably simple: avoid smoking.24
Breech presentation at term and external cephalic version
At term, 3-4% of all babies will present by the breech. The recent term breech trial showed a notable increase in perinatal mortality and morbidity when a vaginal delivery is planned, providing unequivocal evidence that women with a breech presentation at term who plan a caesarean section will have a baby less likely to die or have a serious outcome.25 Women who plan a vaginal delivery will have a 1% increased risk of perinatal death and a 2.4% increased risk of serious neonatal morbidity. Caesarean section is, however, associated with a small increase risk of maternal morbidity (relative risk 1.29, 95% confidence interval 1.03 to 1.61).26 External cephalic version for breech at term will reduce non-cephalic births by nearly 60% but is not offered universally.27 A need therefore exists to implement this simple, apparently safe, alternative to the planned caesarean section in all obstetric units and offer it universally.28 A planned caesarean section with its increased maternal morbidity should not be the first or only obstetric intervention for the term breech.
Reducing operative deliveries
Trial of scar
Concerns have arisen that the rate of caesarean sections has been increasing steadily over the past two decades; the results of the term breech trial will be an added pressure on this. The National Sentinel Caesarean Section Audit Report in 2001 (www.rcog.org.uk) showed that in the United Kingdom, 21.3% of women now deliver by caesarean section, a similar rate to the United States. This rate has almost doubled in the past decade. The audit commission has estimated that every 1% increase in the rate of caesarean sections costs the NHS an additional £5m ($8m; €7m). Even elective caesarean sections, which are recognised to be the safest, probably have at least a doubling in risk of maternal death.8 Research has therefore recently focused on the safety of a vaginal delivery after a previous caesarean section and in what circumstances it should be encouraged.
Some 80% of women will achieve a vaginal delivery after a previous caesarean section, even when the cause of the original operation was well defined cephalopelvic disproportion.29 Reasonable retrospective evidence now supports the commonly held belief that both the interval between pregnancies (> 6 months) and a previous vaginal delivery reduce the risk of scar failure.30 31
The chance of successful vaginal delivery is, however, reduced to 60% if labour is induced.32 Rupture of the scar occurs more commonly in these women (1 in 50 women induced with prostaglandins, compared with 1 in 200 if the labour is spontaneous).33 This study of more than 20 000 women with one prior caesarean section defined outcome accurately; only one in 20 scar ruptures caused fetal death. Therefore the overall fetal mortality associated with a trial of scar is extremely small and comparable to the risk of an intrapartum stillbirth in all women (1 in 1500), assuming safe intrapartum management. Only a minority of women with ruptured scars require a hysterectomy (4.4%) and other serious morbidity such as infection, bladder injury, or paralytic ileus occurs in fewer than 10% of women. These data support the policy of encouraging women to deliver vaginally after one previous caesarean section, which is probably the single most important intervention to prevent caesarean section rates escalating further.
Intrapartum care
The recent increase in operative intervention has not been associated with improved perinatal morbidity or mortality. Increasing expectations and medicolegal fears probably contribute to iatrogenic morbidity in pregnancy. Routine investigations in all women are known to increase intervention, sometimes without clear benefit. An example of this is the routine use of electronic fetal monitoring, which is now not recommended in women at low risk. A cardiotocogram performed on admission in women at low risk was assumed to be desirable to identify fetuses at risk. A recent randomised controlled trial comparing this with Doppler auscultation has shown that cardiotocograms result in a notable increase in intervention, including oxytocin augmentation and use of epidurals, and cause an increase in operative deliveries without any evidence of improvement in the wellbeing of the newborn. Given the number of women involved in this intervention, withdrawing the routine use of the cardiotocogram on admission is likely to reduce unnecessary intervention considerably.
Where available, more than one in five women will request epidurals for pain relief in labour. These are associated with longer labours, more use of oxytocin, and increased operative vaginal deliveries.34 Low dose epidurals are being used increasingly, which allow some mobility while maintaining adequate analgesia. This is achieved by adding opiates and reducing the bupivacaine dose. A recent randomised controlled trial has shown that low dose epidurals reduce the need for operative vaginal deliveries, so that one in four could be prevented.35 Several studies have also shown that women prefer them, so there seems little justification in continuing to use the higher dose procedure.
Additional educational resources
www.cemach.org.uk/—The new Confidential Enquiry into Maternal and Child Health (CEMACH) was launched in April 2003. It was founded on the Confidential Enquiry into Maternal Deaths (CEMD) and the Confidential Enquiry into Stillbirths and Deaths in Infancy (CESDI) and is part of a strategy for the development of the national confidential enquiries being implemented by the National Institute for Clinical Excellence (NICE). CEMACH has a wider brief to include children up to the age of 16 years and its aim is to improve future care of mothers, babies, and children.
www.rcog.org.uk—RoyalCollege of Obstetricians and Gynaecologists. The RCOG is dedicated to the encouragement of the study and the advancement of the science and practice of obstetrics and gynaecology
www.bapm.org.uk—British Association of Perinatal Medicine, aims to improve the standard of perinatal care in the British Isles.
www.nice.org.uk—National Institute for Clinical Excellence, set up as a special health authority for England and Wales on 1 April 1999. It is part of the National Health Service (NHS), and its role is to provide patients, health professionals, and the public with authoritative, robust, and reliable guidance on current best practice.
www.nelh.nhs.uk—The National Electronic Library for Health programme is working with NHS libraries to develop a digital library for NHS staff, patients, and the public.
www.apec.org.uk—Action on Pre-eclampsia (APEC) is a UK charity set up in 1991 to ease and prevent suffering from pre-eclampsia and improve care and understanding of the condition.
www.tommys.org—Charity that funds a national programme of research, education, and information aimed at understanding and preventing premature birth, miscarriage, and stillbirth.
www.bmfms.org.uk—The British Maternal and Fetal Medicine Society aims to provide a forumwhere issues of relevance to obstetricians and other professionals involved in problem pregnancy care are discussed, to encourage improved standards of care.
Footnotes
-
Competing interests None declared.