Article Text

Statistics from Altmetric.com
Introduction
Determining if a particular treatment improves important clinical outcomes such as symptoms, overall quality of life, incidence of CVD, mortality, among others typically requires well-designed randomised clinical trials. Once this type of evidence is available, clinicians can then use these treatments in day-to-day practice. Hopefully, we would all agree that almost all day-to-day healthcare decisions should be made at the level of each individual patient. Given that, we are becoming increasingly uneasy observing that evaluations of the impact of evidence-based practice (EBP) are invariably focused on improving population-level health outcomes (overall incidence of heart attacks or hospitalisations) rather than at the individual patient level.
We believe this focus is inappropriate and fundamentally flawed for the following reasons.
Population-level health outcomes rarely if ever take into account patient values and preferences and therefore by definition fly directly in the face of the fundamental goals and definition of EBP. Ignoring patient values and preferences or at least not placing them at the forefront of decision making legitimises the argument that the presence of effects at population levels is sufficient justification for recommending treatments even though the absolute magnitude of these changes clearly may not be important to all individual patients.
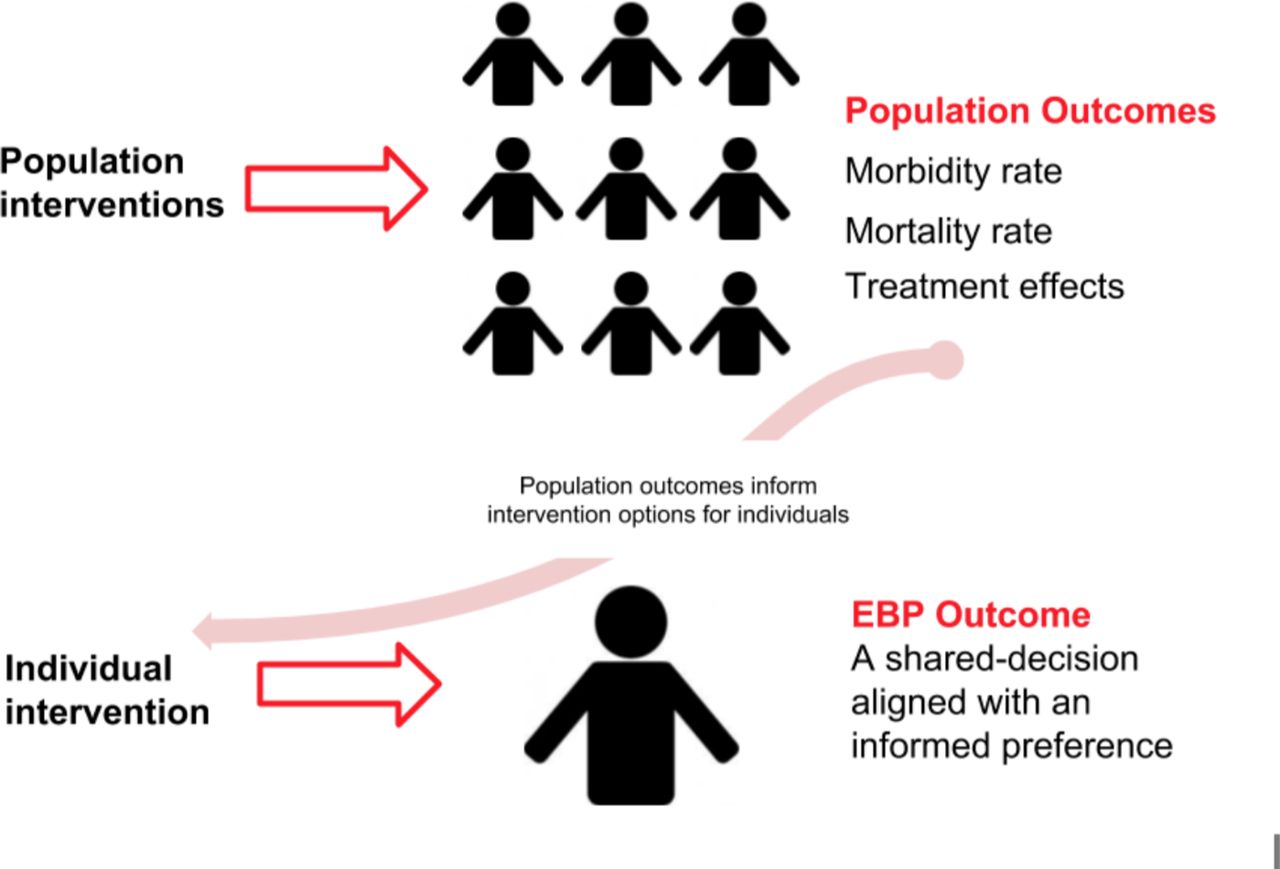
It seems a frame-shift has taken place, where population-level metrics are being applied in error to a phenomenon that should be evaluated at an individual level. Figure 1 illustrates the two frames—one where interventions should, correctly, be evaluated by population-level outcomes, including morbidity, mortality and treatment effects, and the other showing that at the level of individuals, the right outcome is whether a decision informed by the best available evidence is aligned to a patient’s informed preference.
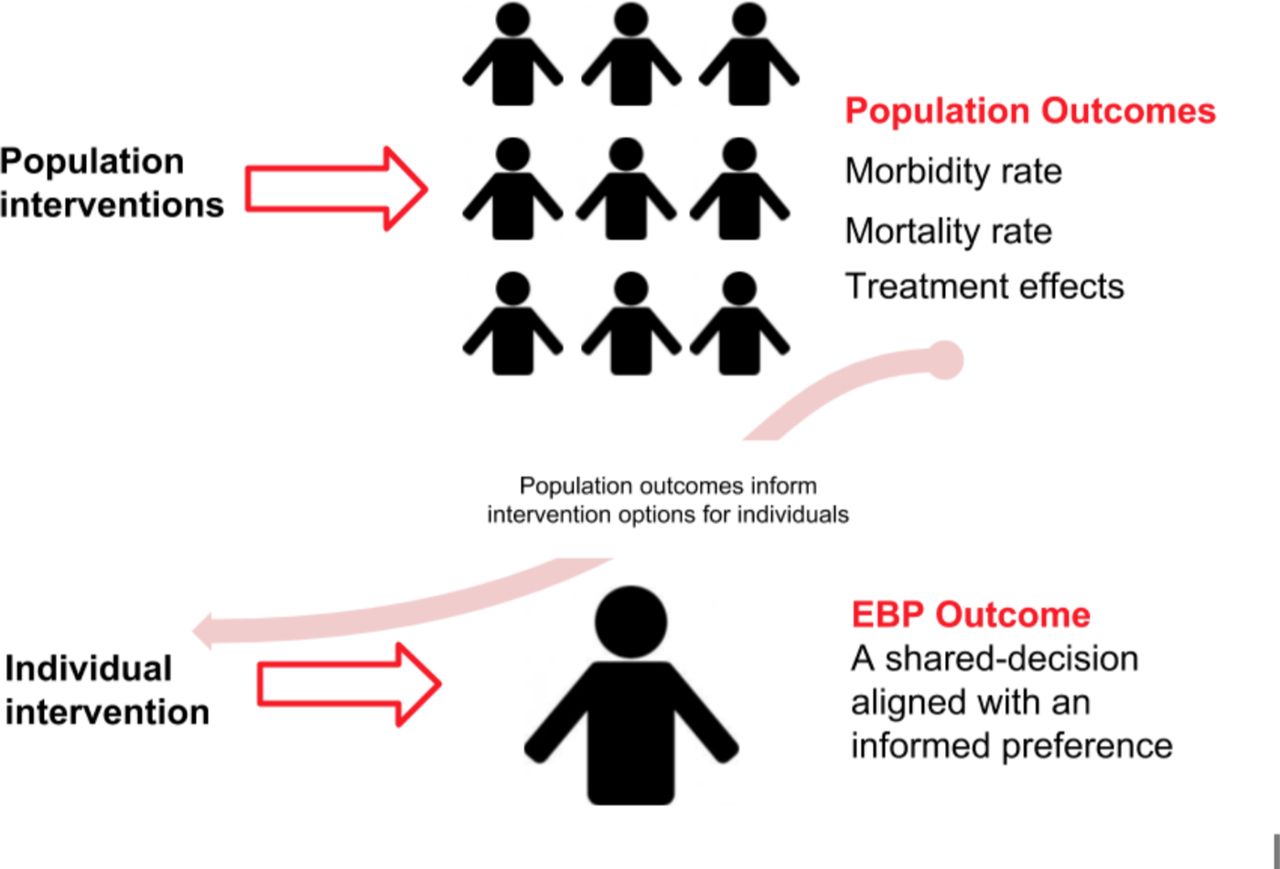
To avoid continuing this individual-to-population frame-shift error, we suggest the key outcome for EBP evaluations should be primarily if not almost exclusively focused on shared decision making (SDM). SDM in this context is defined as a process in which clinicians and patients collaborate, where the best available evidence is shared, and the informed preferences of patients are respected.
Our reasons for suggesting such a solution follow.
How we came to ask the wrong question
Ever since the introduction of the evidence-based medicine paradigm, there has been a need for proponents to try to explain EBP’s philosophy to detractors. In 1996, Sackett et al penned an editorial entitled Evidence based medicine: what it is and what it isn’t. 1 In 2014, Greenhalgh et al asked whether Evidence-based medicine is a movement in crisis?,2 saying how EBP has been ‘misappropriated and distorted by vested interests.’ and real EBP needs to ‘Make the ethical care of the patient its top priority’.
People have often argued against EBP by asking what they think is a clever question: ‘Is there really any ‘evidence’ that EBP improves outcomes’. Such a question leads to an examination of trial evidence; arguments about conflicting data or even the examination of high-quality, systematic reviews. But the arguments that typically follow are based on flawed comparisons. Effect sizes from scientific studies are important of course; but they are only one element in making a decision at the individual level. People will make entirely different decisions when faced with exactly the same evidence because people will form different preferences and, by definition, EBP rests on respecting the informed preferences of individuals.
The individual-to-population frame-shift error
All of these examples reveal a fundamental misunderstanding many have about EBP: that the rationale and justification for EBP relies on being able to demonstrate that EBP somehow should lead to better clinical outcomes. This common misunderstanding pervades the current scientific discourse around EBP and impedes how, as a society, we should practice medicine. EBP is about taking care of individuals and is not about the insensitive use of population-based evidence. As soon as the question moves to one of clinical outcomes, this individual-to-population frame-shift occurs and clinicians often consider scientific probability at aggregate levels. Looking at outcomes for individuals is entirely different from thinking about evidence from large groups in trials and in cohorts.
EBP versus population outcomes
EBP has become the dominant discourse in healthcare and many educational curricula have adopted its central ideas. Unfortunately, clinical practice guidelines which profess to be based on EBP concepts seem to primarily focus on population-based outcomes. To clarify our argument, it is important that we outline clearly what EBP ‘is’ and what EBP ‘is not’ (see figure 2).

{kind=link}
{kind=link}
EBP has been defined simply as the integration of the best available evidence with clinical expertise and patient preferences.1 EBP is not about slavishly following clinical practice guidelines and, therefore, EBP is not about solely following the result of the best randomised controlled trial nor the most recent systematic review.3 Trustworthy clinical guidelines should be valuable distillations of scientific evidence, but guideline writers rarely go the necessary extra step of showing how to personalise the evidence to the individual patient, who likely differs from the typical patients enrolled into studies and certainly has unique preferences and priorities that require consideration.4 Because it may be impossible for guidelines to elicit and integrate all individual preferences, guideline writers need to explicitly acknowledge the concepts of SDM throughout the guideline and within each recommendation. To do this, they need to provide information that helps people compare reasonable options rather than describe specific thresholds for treatment. Guidelines may need to become similar to patient decision aids and focus more on providing the user with useful evidence-based estimates of benefits and harms to facilitate SDM.5
EBP is not about checking boxes; real people do not fit into boxes: they have goals, idiosyncrasies and live in complex relationships and contexts which will inevitably shape decisions and actions. EBP is also not about having zero competing interests. We all have interests, whether professional, intellectual, financial or personal; therefore, because these interests will influence our decisions they need to be made known.
EBP is definitely not about ignoring basic science, which is the groundwork for many advances in medicine and EBP is not something new: Archie Cochrane drew attention to the need to make better sense of the scientific evidence over 40 years ago.3
Fundamentally and noteworthy, as resources become constrained, EBP is also not about rationing care or saving money.
Finally and critically, EBP is not solely about having a positive effect on health outcomes. Clearly, health outcomes such as mortality, cardiovascular disease, quality of life, among others are very important, especially when assessing the effect of treatments, policies and screening programmes at population levels; the scientific evaluation of these outcomes is invaluable. However, aggregate health outcomes may not be important when assessing EBP at the level of individual patient care. The main reason these potential rationales are somewhat irrelevant to individual patient care is that EBP is fundamentally about accomplishing SDM. SDM is defined as a process where clinicians support and respect patients’ well-informed preferences and where preferences are based as much as possible on high-quality evidence.
To illustrate, the following hypothetical RCT could be an example where following EBP might lead to worse population clinical outcomes at individual levels, but which are entirely reasonable, if we honour the views of informed patients.
Imagine an RCT of statin use in primary prevention, where people are randomised to (1) being advised to take a statin or (2) where patients were informed and supported to make a choice about taking a statin (in other words, EBP). In this hypothetical RCT, to illustrate our point, let us assume:
statins reduce the risk of heart attacks and strokes by approximately 25% (relative reduction) over 5 years. In a patient with an absolute 5 year cardiovascular risk of 4%, taking a statin would reduce their absolute risk from 4% down to 3%, an absolute benefit of 1% over that time period.
a substantial number of people, when given this data about absolute benefit, will decide NOT to take a statin pill every day for 5 years, irrespective of other issues like side effects. In their view, the size of the gain (1% absolute benefit) is not worth the effort and burden of taking the treatment.
Given this, fewer people in the ‘make a choice’ (EBP) group would take a statin than those in the ‘just take a statin’ group. Therefore, if in fact statins reduce the risk of cardiovascular events on a population level, the people randomised to the ‘make a choice’ group would end up having more heart attacks and strokes because fewer were on a statin than in the ‘just take a statin’ group. In other words, supporting a shared decision would lead to ‘worse’ outcomes at a population level and some might conclude therefore that EBP is ‘not effective’ and maybe even harmful.
So assuming this was the outcome of this hypothetical RCT, does that mean doing EBP is misguided? Of course not. Is it an error for an individual to choose not to take a regular medication because they value being free of the nuisance and possible side effects more than the 1% 5 year risk reduction? Definitely not. The outcome that really matters is whether SDM occurred and the individual’s informed preference was respected. As clinicians, we should be agnostic, where ethical to be so, as to the choice made by the patient. It would be fascinating in this example, to measure higher confidence with a decision made, greater immunity against future regret and higher perceived health happiness and see if these were different across the two groups.
Of course, there are exceptions to this way of thinking but these exceptions in no way detract from the central tenet of the argument but rather, these exceptions are examples of societal norms intervening to protect against vulnerability. For example, in most societies, laws prevent harm from occurring, where mental incapacity or strong personal beliefs may threaten the well-being of others. Jehovah Witness’ refusal to transfuse blood to those in dire need is a well-known example where courts intervene to safeguard life. Other examples include involuntary detention for psychiatrically unstable patients who risk harming themselves or others, surrogates are asked to make decisions for those people truly unable to consent to treatment in immediate life-threatening situations and possibly smoking bans that lead to important reductions in morbidity and mortality. An intriguing example that some would consider an important exception is mandatory vaccination with the potential of herd immunity. In this case, a shared decision not to be vaccinated for a transmissible disease could lead to inherent harm of others. All of these can and have been debated. As healthcare professionals, we are all also aware of patients who prefer to avoid taking responsibility for decisions by asking their healthcare professional, ‘Well, what would you do?’ and who are willing to follow their recommendation. Overall, it seems many of these exceptions are based on the principle that one can be free to make up one’s own mind but not always if it has the potential to do significant harm to oneself or to others.
Finally, in a healthcare system where most costs may be met by the state, many would appropriately suggest there may be a duty to ensure funding is spent wisely. Meeting this obligation may, in some situations, influence the imperative to allow an informed preference to be the only outcome that can be considered.
Making SDM the key outcome for EBP
Given that honouring patient preferences is part of the EBP equation, it follows that an insistence on beneficial population-level health outcomes is illogical. The solution to this misappropriation and misinterpretation of the EBP concept is to make shared decision the primary outcome evaluated when we consider healthcare provision to individuals. Given this suggestion, it is important to understand the full implications of this way of thinking. This is not easy work—it takes care and kindness to make sure patients are supported to become well-informed and confident enough to voice their personal preferences. Forming this sort of partnership with patients is skilled work and calls for deliberation and collaboration.4
However, it is important to realise that making informed choice the primary outcome comes with complications and may be potentially disruptive. Clinicians across the globe are influenced by the dominant outcomes-driven narrative that patients should be recommended treatments proven to improve population-based outcomes. Some even consider recommendations in guidelines to have legal force and that they could be open to litigation if they do not explicitly follow population-derived treatment recommendations. However, some guidelines now explicitly state that guidelines should not be used as a legal resource in malpractice cases.5 In addition, many courts in a number of countries are now stating, ‘The reasonable-patient standard … requires physicians and other healthcare practitioners to disclose all relevant information about the risks, benefits, and alternatives of a proposed treatment that an objective patient would find material in making an intelligent decision as to whether to agree to the proposed procedure’6—in other words, a standard that requires SDM. The real test of patient centeredness would be the respect shown to patient’s informed preferences. Payment for performance frameworks that have explicitly reified healthcare outcomes, such as direct payment for achieving cohorts of patients with blood pressures or glucose measurements under prescribed thresholds, fly in the face of respecting and accepting that some patients will make contrarian decisions once provided with the absolute cardiovascular benefit associated with lowering surrogate markers.7 If this is the case, then assessments of the impact of EBP can be simplified to answering the question: did SDM occur or not?
Evaluating EBP decisions—N always=1
As healthcare professionals, we accept the need to explain to patients there is evidence of effective treatments at population levels. However, the decision whether to adopt most treatments at an individual level is a decision that is unique, context-based and derived by careful deliberation about trade-offs. This careful deliberation defines EBP, and in the vast majority of circumstances, the only outcome of relevance for EBP is to measure whether a shared decision was made.
Footnotes
Contributors JM and GE contributed equally to the writing of this article.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.