Article Text

Statistics from Altmetric.com
Emollients are readily available in prescription and over-the-counter products, and are commonly used in homes and healthcare facilities. These products are not harmful or flammable in isolation, but if they are combined with flames, such as the light of a cigarette, and fabric, they accelerate fires, resulting in burns and deaths. This article describes a prevent future death case report of a 74-year-old woman who succumbed to burns in the presence of paraffin based emollient creams and a lighted match. We highlight the fire risks of such products and the need for greater awareness among the public and healthcare professionals.
This article is part of the coroners’ concerns to prevent harms series.1 It discusses a prevention of future death report on the fire accelerant properties of emollient products.2
Products containing emollients, from E45 and Vaseline to Cetraben, are widely available over the counter or by prescription. In the past 12 months (October 2019 to September 2020), more than 15 million items containing emollients were dispensed in England, costing more than £93 million.3 They come in various formulations, including liquids, creams and ointments (box 1), and are used to hydrate the skin. Emollients can contain paraffin, an oily liquid composed of saturated hydrocarbons from petroleum,4 to help form a protective film over the skin and trap moisture. Paraffin is cheaper than alternative agents, such as lanolin or olive oil.5 If their residue on fabric is exposed to fire (eg, from the light of a cigarette or stovetop), emollients (both paraffin free and paraffin based) can act as accelerants to the fire, and have devastating consequences. It was previously thought that the risk of fire was posed only by emollients containing more than 50% paraffin, but it has been acknowledged that the fire risk cannot be excluded in non-paraffin based emollients.6 7 Thus the lack of awareness of the fire risks may cause further harm.
Evidence-based medicine facts: paraffin based emollients23
Formulations
Liquids
Creams
Ointments
Gels
Dressings
Sprays
Ingredients
Paraffin derived components, which may include:
white soft paraffin
liquid paraffin
liquid paraffin light or
yellow soft paraffin.
Certain formulations may contain one or more of the following:
alcohols and acids: benzyl alcohol, cetostearyl alcohol (including cetyl and stearyl alcohol), wool alcohols, isopropyl palmitate, isopropyl myristate and sorbic acid
salts: disodium edetate, magnesium sulfate, sodium lactate and sodium pidolate
preservatives: chlorocresol and phenoxyethanol
parabens: hydroxybenzoates
emulsifiers: polysorbates or emulsifying wax
diols: propylene glycol
lanolin or wool fat
antimicrobials
soya oil and
fragrances.
Indications
Dry skin conditions
Eczema
Psoriasis
Ichthyosis
Burns
Pruritus
Hazards and harms
Severe and fatal burns due to accelerant properties
Allergic skin reactions
Aggravation of acne
Folliculitis
Falls, if applied to areas that make surfaces slippery
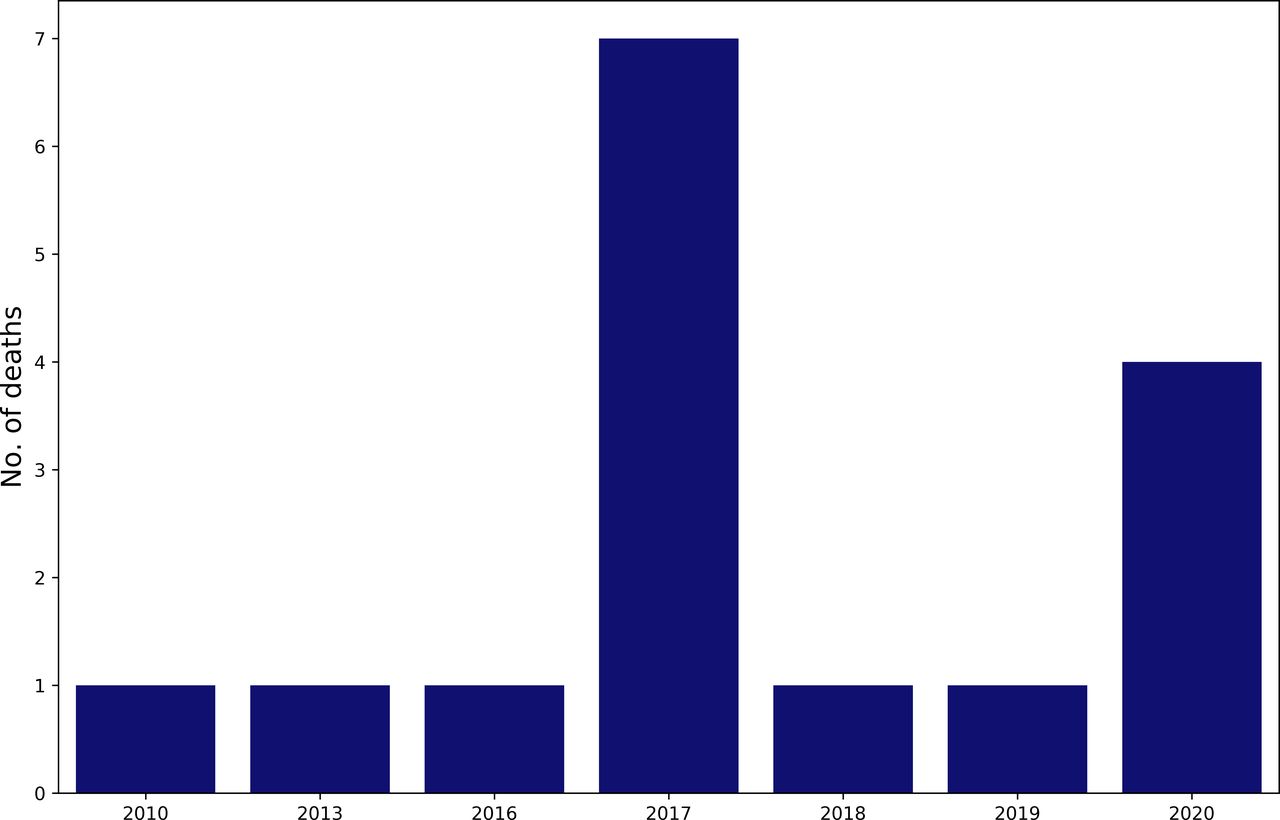
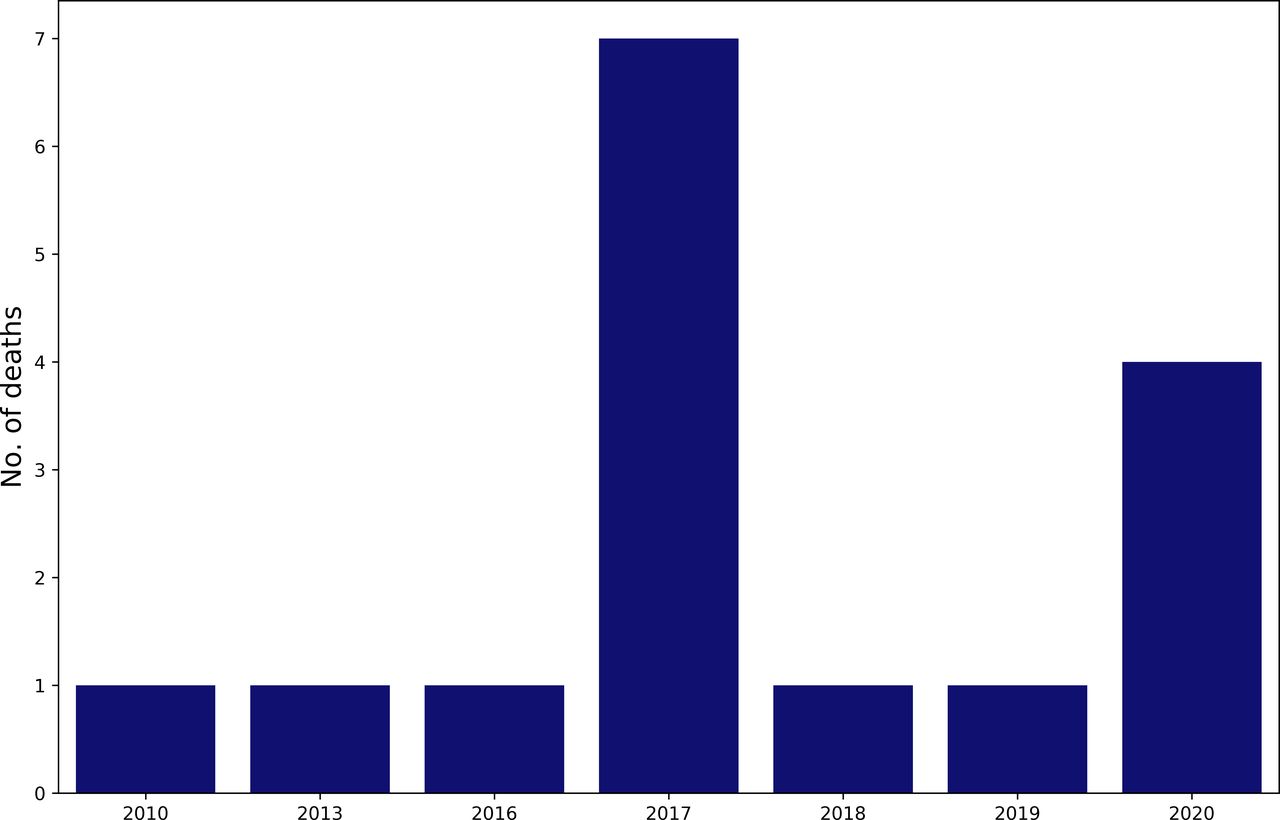
Sixteen deaths from severe burns linked to the accelerant properties of emollients have been reported in the UK (figure 1). In December 2018, the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) reported 11 fatal burn injuries from paraffin based emollients, and the Fire and Rescue Services reported 50 fire incidents (49 fatal) involving paraffin based emollients between 2000 and 2018.7 Updated data from the MHRA identified five additional fatalities since the 2018 report (figure 1).8 Others have highlighted the fire hazards of using these products, and the need to share information for patients.9 10 In this Coroners’ Concerns to Prevent Harms article, we identify a preventable death from paraffin based creams2 and explore how to reduce their harms.
{kind=link}
Numbers of deaths from fires or burns relating to emollients, both paraffin based and paraffin free, reported to the UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) yellow card scheme between 1 January 2010 and 27 October 2020. There were 18 reports in total with 16 fatal and two non-fatal outcomes. Data were obtained through a freedom of information request to the MHRA.8 Pandas, Seaborn, and Matplotlib packages in Jupyter Notebooks (Python V.3) were used to create the plot. The data and code are openly available on our Github.24
An accidental death
In 2019, a 74-year-old woman was pronounced dead in her home after neighbours alerted emergency services to a potential fire. Investigations revealed that the fire had been caused when the deceased used a match to light a cigarette. She had used a paraffin based emollient cream, but the indication for its use was not mentioned in the coroner’s report. She was known to be a heavy smoker, and the paraffin based cream probably soaked her clothing, acting as an accelerant for the fire. One month before her death, her carers, who were concerned about the risk of fire, had made a safeguarding referral. However, no actions were taken to mitigate harms prior to her death. A low level of carboxyhaemoglobin was identified in the toxicology analysis, and burns were listed as the cause of death. The coroner concluded the inquest as an 'accidental death’.2
During the inquest, the coroner raised several concerns surrounding a lack of awareness of the fire risk of paraffin based creams by healthcare professionals, carers and the public (box 2). The coroner addressed these concerns to six organisations, including: the Department of Health and Social Care, the National Institute for Health and Care Excellence (NICE), Public Health England, the British Medical Association, the Care Quality Commission, and Trent and Dove Social Housing. To date (January 2021), three organisations have responded.
Coroner’s concerns2
Fire investigators reported attending an increasing number of fires involving mostly elderly residents where paraffin based creams were in use.
Several creams containing paraffin are readily available in both prescription and over-the-counter products.
When applied to the skin, they also come into contact with clothing, and may not be washed away in a normal washing cycle, leading to greater contents in clothing.
If the paraffin causes a fire on clothing, the outcome is highly likely to be lethal, rapidly engulfing the victim in fire, with death being primarily due to burns rather than smoke inhalation.
There is a lack of awareness of the fire risk of such creams by healthcare professionals, carers and the public. Awareness needs to be raised among healthcare professionals and others who may prescribe or sell paraffin based products or care for someone using them.
The Department of Health and Social Care responded on 21 January 2020 (due 17 January) and described previously seeking advice from the MHRA, which resulted in a drug safety update in December 20187 and an in-depth review by the Commission on Human Medicines (CHM). In its response, the department also noted that the review by the Commission on Human Medicines led to two meetings with stakeholders to design resources and methods for their distribution in the form of a toolkit, which was published in July 2020,11 alongside a press release about the new campaign.12 13 Despite various efforts to share information about the risks, fatalities from fires associated with emollients continue to occur.
Safe use of emollients
Emollients are not spontaneously flammable, and they should not be discontinued based on the fire risk alone. The dangers arise when emollients are absorbed in clothing, bandages, bedding or furniture, and are combined with an ignition source. People who use large volumes of emollients, apply products often and to large surface areas; those who smoke, and people exposed to open flames (eg, when smoking or cooking), are at the greatest risk of harm, which appears to be unrecognised in the community.
Successful burn prevention programmes have combined education, product design change and legislation to prevent harm.14 Product design change was instigated in 2018 when legislation was implemented requiring all paraffin containing emollients to display warning labels, and the 2020 MHRA campaign focused on education.7 In isolation, these measures may not be as effective in preventing harm. Therefore, it is important to implement a multi-pronged approach that educates the public and healthcare professionals, uses product design change in leaflets and warning labels, and critically appraises these methods to ensure evidence-based policy decisions are made going forward.
Current measures to prevent harms may be insufficient. Since this prevent future death report was issued by the coroner (November 2019), four further deaths involving emollients have occurred (figure 1). Other aspects to consider in the prevention of harms from emollient related fires should include ongoing education, targeting high risk groups and the provision of better evidence related to the fire risks posed by emollients, including effective methods of prevention. While the resources provided by MHRA are freely available, their success in raising awareness among the public has not been appraised. Although emollient products contain written information and safety warnings on labels, this may be insufficient as users may not read this information.15 In addition, the MHRA campaign does not focus on targeting those at high risk of emollient related fires.
It is necessary for high risk persons to be actively identified at the point of prescribing, dispensing or purchasing emollients. However, some groups at risk may require additional actions, such as referral to a ‘stop smoking’ service or a fire safety assessment. Relevant government agencies should consider intensifying their efforts to distribute information to patients and highlight the importance of this risk to healthcare providers, which may be lacking in healthcare settings. For this to be successful, a national approach should be considered that will cascade down to the local level. In a busy clinical environment, alerts and checklists with relevant questions to identify high risk patients should be considered. The National Pharmacy Association created such a checklist in 2008, but it is unclear how widespread its use is to date.16
Emollients are the first line treatment for many dermatological conditions, and their importance in managing these conditions should not be overshadowed by their risk of accelerating fires.17 It should also be noted that other paraffin containing products, such as some topical antibiotics, may pose a similar risk, and preventative measures should be considered while ensuring the continued safe use of these products. While efforts are being made to raise public awareness of such harms through the media,18–22 actions to prevent future deaths are needed. For informed consent to occur, patients must be made aware of the risks, and healthcare professionals recommending or prescribing emollients must ensure patients are provided with this information. The public should also be encouraged to report harms to the yellow card scheme to ensure accurate monitoring of suspected harms. To date, third party organisations concerned with dermatological conditions and burns have not played a major role in educating the public about the risks of emollient related fires. These organisations are experienced and well placed to spearhead a collaborative effort to raise awareness and prevent harms.
Footnotes
Twitter @Richards_G_C
Contributors MKB identified the prevent future death case reports, conducted a systematic literature search and wrote the first manuscript draft. GCR submitted the freedom of information request for the data on the number of deaths from emollient related fires and burns, analysed the data, and edited and contributed to the manuscript drafts.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GCR is financially supported by the National Institute of Health Research (NIHR) School for Primary Care Research (SPCR), the Naji Foundation, and the Rotary Foundation to study for a Doctor of Philosophy (DPhil/PhD) at the University of Oxford. GCR is the editorial registrar of BMJ Evidence-Based Medicine, founded the Coroners’ Concerns to Prevent Harms series and is developing the preventabledeathstracker.net. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Provenance and peer review Not commissioned; externally peer reviewed.