Article Text

Statistics from Altmetric.com
Introduction
The flipped classroom model is a well-known evidence-based educational approach for student-centred learning. In a flipped classroom, students receive instructional content before class, and use classroom time to engage in assignments and discussions. Studies have shown the flipped model to result in comparable1 2 or better3 4 outcomes compared with a traditional lecture-based model. A meta-analysis in 2018 found a significant effect favouring the use of a flipped classroom model with videorecorded lectures as part of preclass materials, for graduate-level healthcare education compared with traditional instructional models4.
The flipped class model is in line with educational theory for adult learners, or androgogy,5 which posits that effective educational experiences are those that actively incorporate the learner. The flipped classroom promotes self-directed learning during knowledge acquisition followed by interactive problem-based assignments in which the learner applies knowledge acquired during self-study.6
In most of the recent studies on the flipped classroom, the preclass materials were accessed via online learning management systems or websites, and the class meetings were typically completed in a physical classroom setting. However, healthcare programmes are beginning to move toward online/distance learning models, in which most—if not all—interactions occur online. As universities continue to expand the availability of online healthcare degree programmes, educators of evidence-based practice (EBP) courses may soon face the task of redesigning their courses for an exclusively online experience. It is important to address the question of whether online learning experiences in EBP education can produce equivalent results to those seen in long-established on-campus teaching models.
In 2017, the University of Southern California (Los Angeles, California, USA) Division of Biokinesiology and Physical Therapy initiated a hybrid (online/on-campus) pathway of their long-standing on-campus Doctor of Physical Therapy programme. Thus, each course in the programme was translated to accommodate students in the hybrid pathway. An EBP course that had been taught on-campus in a flipped classroom model since 2011 was translated to an exclusively online flipped classroom model in 2018.
To date, we have not identified studies that compare EBP education online in a flipped classroom model versus on-campus in a flipped classroom model. In this study, we describe a flipped classroom EBP course and assess outcomes among students enrolled on the traditional on-campus version versus those who attended their class meetings online.
Methods
Design
This was a controlled comparison between an on-campus and online flipped classroom EBP course.
Study population
This study assessed graduate students (n=142) admitted to either the online (n=46) or on-campus (n=96) pathway of a Doctor of Physical Therapy programme. Admission criteria were consistent between the two pathways. Students were enrolled in a required EBP course in their first year of a 3-year professional education programme.
Intervention
Students participated in a 16-week course (January–May 2019) covering the five steps of EBP.7 These five steps are explored through the lens of physical therapist practice, with case scenarios involving common conditions seen in physical therapy settings. The course curriculum aligns with the American Physical Therapy Association’s EBP curriculum guidelines,8 see table 1.
Course content and student performance for the five steps of evidence-based practice
The course used a flipped classroom format. Students completed instructional content online before class, then during a weekly class meeting, worked on assignments in small groups with instructor support. The preclass instructional content was comprised of a patient case video, short videorecorded lectures, review and reflection questions, and a research article pertaining to the patient case.
Patient case videos
In the video-based patient cases, a physical therapist interviews a professional actor who plays a patient with a simulated health condition (figure 1). Through the interview, students are introduced to an area of clinical uncertainty that can be formulated into a searchable clinical question. Four cases were developed for use in one or more weeks during the course. The studio-produced patient case videos allow students to experience (1) the physical therapist interview and patient history taking (2) the emergence of clinical uncertainty in a realistic scenario and (3) use of the five-step EBP framework to address clinical uncertainty in patient care.

Screenshot from a patient case video. A physical therapist models the patient interview with a professional actor who played a patient with a simulated health condition. Through the interview process, the students are introduced to an area of clinical uncertainty that could be formulated into a searchable clinical question.
Videorecorded lecture content
The videorecorded lecture content builds on the patient case scenarios to introduce EBP topics. Lecture videos were filmed in high-definition and framed so that lecturer and slide content were visible on screen simultaneously and legibly (figure 2). The lecture slides were designed to be in line with evidence-based guidelines for multimedia content.9 The video lecture content was broken into 15 total modules, each containing a series of short videos 5-10 minutes in length, consistent with recommendations for video content duration to maximise student engagement.10 Each module contained an average of 11±6 videos, with average viewing time of 46±23 minutes per module.

Screenshot from the videorecorded lecture content. Videos were filmed in high-definition and framed so that lecturer and slide content were both visible on screen.
The course material was hosted on a web-based learning management system. Students were required to complete 1–2 preclass learning module(s) per week prior to their scheduled class meeting. The learning management system allowed students to pause and replay the video content, alter the viewing speed, toggle closed captioning on/off and adjust videoresolution. Copies of lecture slide content were provided to students to facilitate notetaking. Course instructors monitored students’ weekly progress through the learning management system prior to the weekly class meeting to ensure that the educational content was delivered as planned. Students were contacted via email if they did not complete weekly content as assigned.
Review and reflection questions
Review and reflection questions were embedded between video lecture segments. These low-stakes formative practice questions are used to test students’ recall and to promote reflection on topics covered in the video content (figure 3). Question formats are either multiple choice, matching or open-ended response. For multiple choice and matching, students select the correct response before proceeding to the next video segment. Faculty reviewed the open-ended response questions prior to the weekly class meeting and provided individualised and/or group feedback on questions during the weekly class meeting. Each module has an average of 5±6 multiple choice/matching questions and 5±5 open response questions, with estimated average student engagement time of 31±28 min per module.

Examples of review and reflection questions embedded between video lecture segments. The low-stakes formative practice questions are used to test students’ recall and to promote reflection on topics covered in the video content. question formats are either multiple choice, matching or open-ended response.
Research article
Students were assigned one research article to read each week that related to the clinical question posed in the patient case video. Articles were selected based on their applicability to the patient case scenario and the characteristics of the article’s methods and results. Study designs covered in the course include: primary studies (randomised controlled trials and cohort studies), systematic reviews and clinical practice guidelines.
Appraisal assignment
Consistent with the flipped classroom model, students completed an assignment during class meetings that integrated the research article with the patient case and clinical expertise. Each student completed their own assignment but students were encouraged to collaborate among themselves and had frequent faculty input and support during class meetings.
Weekly instructor-led class meetings
Students attended weekly instructor-led meetings that were delivered either: (1) in an on-campus lecture hall or (2) online using video conferencing software (Zoom Video Communications). The instructor to student ratio was 1:32 for the on-campus cohort and 1:12 for the online cohort. To account for the difference in the instructor to student ratio, the length of the weekly meetings was 2 hours for the on-campus class cohort and 1 hour for the online cohort.
Class attendance was mandatory and included an in-class quiz to assess student preparation. Time was allocated for student questions and instructor led content review, followed by small group work to complete the appraisal assignment. Following completion of the assignment, the instructor facilitated class discussion in which students reflected on the research evidence and patient information to determine a plan of care for the patient case.
Instructors
The two instructors (JT and CM) are physical therapists with 15- and 3- years experience teaching EBP. Both instructors had experience teaching the on-campus flipped classroom version of the course, were directly involved in developing the online course materials and led class meetings in the on-campus and online formats.
Outcome measures and data collection
We compared the online and on-campus student cohorts’ performance on a midterm evidence appraisal, the final examination and the total course grade.
Midterm evidence appraisal: The midterm evidence appraisal is a take-home examination conducted independently by each student. The examination requires students to read and appraise an assigned research article and apply it to a provided patient case. Students answer multiple choice and open-ended questions about the applicability and quality of the article, and interpret and apply the study findings. Students are permitted access to online resources but are not permitted to contact other persons in any way (online or otherwise). Academic integrity is addressed synchronously with students on the first day of class, in the two class sessions prior to the exam, in written form on all examination materials and students sign a statement indicating that they are submitting independent work. The assignment is graded out of 70 total points and is worth 20% of the total course grade.
Final examination: The final examination is a 55-point, independent multiple-choice examination based on two research articles that all students are provided 4 days prior to the examination. Students independently answer questions about the articles in a proctored examination. Questions relate to the applicability of the articles to patient care scenarios, the quality of each study’s methods and design, and interpretation and application of the studies’ findings. The final examination is worth 25% of the total course grade.
Total course grade: The total course grade is comprised of all assignments, independent quizzes and examinations. The maximum total course grade is 100%, with a minimum score of 73% required to pass the course.
Data analysis
Descriptive statistics were calculated for the online and on-campus cohorts. Independent t-tests were used to test student performance between the online and on-campus cohorts.
Results
Baseline characteristics of the two student cohorts are described in (table 2). Of the 96 students in the on-campus cohort, 63% were female (mean age=25 ± 3.1), with 100% living within commuting distance to campus. Of the 46 students on the online cohort, 48% were female (mean age=26.7 ± 4.3), with 37% living within commuting distance to campus.
Characteristics of on-campus and online student cohorts
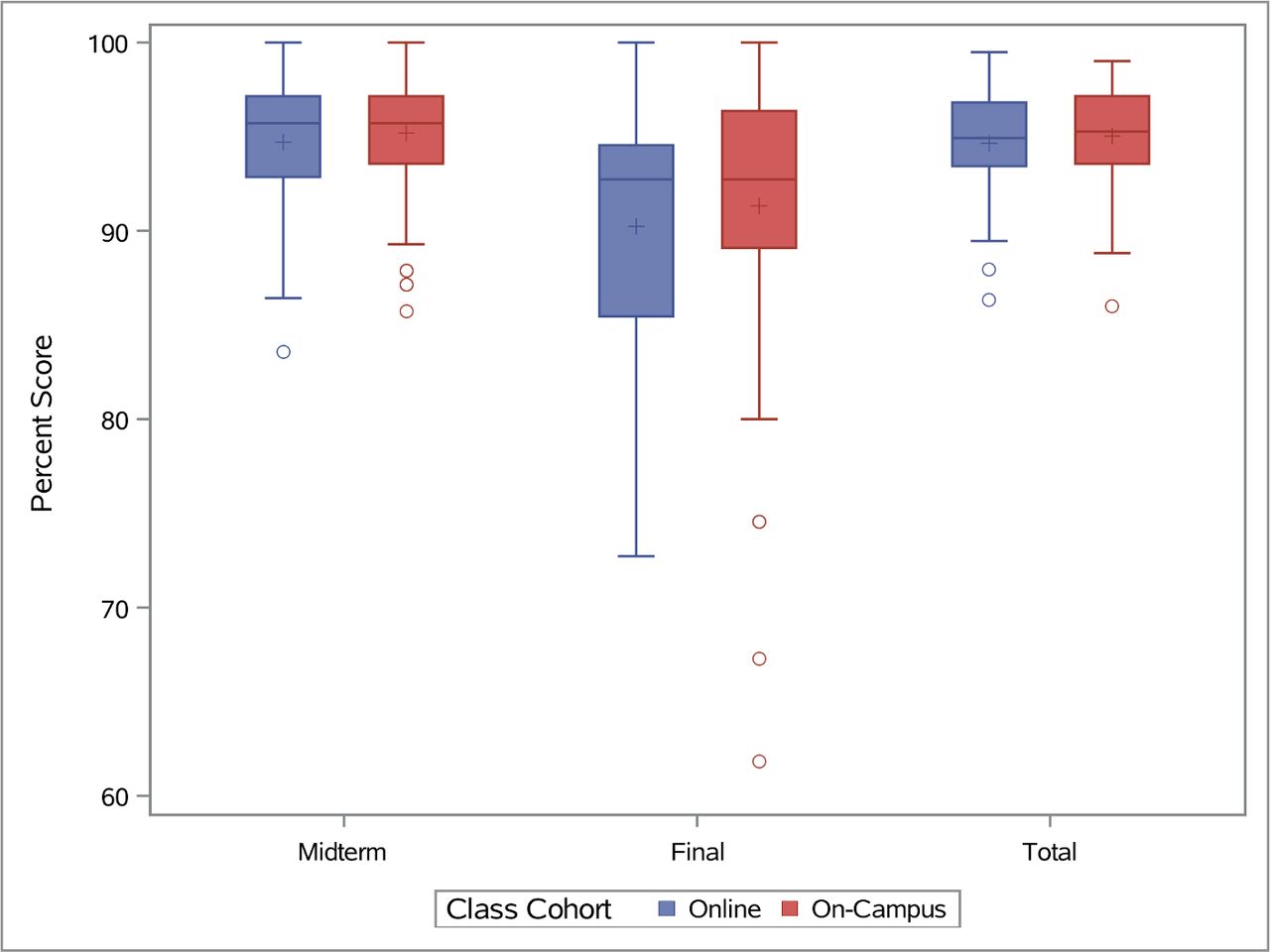
Average scores (SD) for the outcomes of interest are shown in table 3 and score distributions are illustrated in figure 4. There were no statistically significant differences in performance between the on-campus and online cohorts for the midterm appraisal (p=0.41), final examination (p=0.36) or total course grade (p=0.43).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box and whisker plot comparison of the online (n=44) and on-campus cohort (n=96) performance on three course assessments: midterm, final and total course grade. The central box spans from the lower 25th to the upper 75th quartile, the middle line represents the median, the plus sign represents the mean, the whiskers extend from the 10th to the 90 percentile of scores. The circles outside of the box represent outliers.
Results of on campus and online student course assessment performance
Discussion
In this study, we assessed student outcomes in a flipped classroom EBP course designed to be delivered with an online or on-campus class meeting. There was no difference in performance between the on-campus and online cohort. This outcome was consistent with our goal of creating an online experience that would be comparable to our well established oncampus flipped classroom course.
One strength of our flipped class design was that the same preclass materials could be used for the on-campus and online cohorts, so that the only substantial difference was the modality by which class meetings were delivered. The flexibility of this design opens opportunities for EBP education both within and beyond the classroom walls, allowing educators to reach students who wouldn’t otherwise have access to a traditional educational environment.
It should be noted, however, that extensive resources and time were required to create the online flipped classroom course content. Barriers such as these have been cited as points for educators to consider when determining if transitioning from a traditional classroom to a flipped classroom is worthwhile.3 Although startup resources were needed to create online content, we found that once the content was established, both our on-campus and online students were able to benefit from having access to these materials and both performed equally well.
One limitation of this study was that we did not use a standardised assessment of EBP knowledge and skills. However, this study was pragmatic in nature, and the assignments and examinations mirror entry-level physical therapy practice expectations.8 While the midterm examination was fully independent, the final examination method allowed students to collaborate and discuss the assigned articles prior to independently answering a series of multiple-choice questions in a proctored test environment. It is possible that this model could reduce the sensitivity of our outcomes for detecting a difference between groups. Furthermore, the cohort sizes were unequal because the online pathway was established in the past 2 years and is not yet admitting a full class of 96 students. Finally, we did not compare our flipped class model to another model, such as a traditional lecture format. Nevertheless, our controlled comparison gives valuable insight into the capacity for EBP education to be delivered effectively online in a flipped classroom model.
Conclusions
We found that a flipped classroom EBP course delivered with an online or on-campus weekly class meeting resulted in comparable outcomes for graduate physiotherapy students. The benefit of designing a course with online preclass content is that it can be flexibly delivered in person or at a distance, allowing educators to reach students beyond the classroom walls.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the University of Southern California Institutional Review Board (HS-18–00935).
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors CM and JT conceived of the study and implemented it, CM and JT conducted the primary statistical analysis, CM and JT contributed to and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.