Article Text

Statistics from Altmetric.com
Evidence-informed healthcare (EIHC) is a systematic approach to clinical problem solving that facilitates the integration of the best available research evidence with clinical expertise and our patient’s unique values and circumstances.1 To become an EIHC practitioner requires knowledge, skills and practice. The five-step model of EIHC (asking answerable clinical questions, acquiring the evidence, appraising the evidence, applying the evidence and assessing performance as an EIHC practitioner) forms the basis for both teaching EIHC and clinical practice.2
Despite many EIHC success stories, variation in the adoption of evidence-based practice remains a problem.3 Barriers to implementing EIHC are well documented, with lack of resources being the most common barrier,4 followed by lack of knowledge and skills about appraisal, negative perceptions about research, lack of resources and time, low self-efficacy, inadequate access to the literature and financial barriers.4 5 Some of these barriers are directly related to the steps of EIHC, indicating that there is a clear need to improve the teaching of EIHC across all professions.
Interventions using multiple methods are most likely to improve knowledge and skills compared with single interventions or no interventions,6 with the most effective teaching strategies being those that are interactive and clinically integrated.7 Online learning with high levels of interactivity is increasingly used as a learning intervention8 and is as effective a strategy as lecture-based teaching.9 Online learning has the added advantage of providing learner-centred access to course materials at a time and place convenient to them and to tailor their learning to their own timing, pace and needs.8
Virtual patient cases are designed to represent real-life clinical scenarios and are well suited for facilitating the development of clinical reasoning skills,10 an essential element of EIHC. Cases designed using a problem-oriented training approach increase the likelihood of spontaneous analogical transfer of the skills developed.11 As virtual patient cases are already core components of learning in many healthcare professional programmes, we decided to use an online ‘virtual patient case’ approach. We developed modules that offer a simulated learning environment for healthcare students to learn, experience and practice while accommodating for time and geographical constraints.
Module development and pilot testing
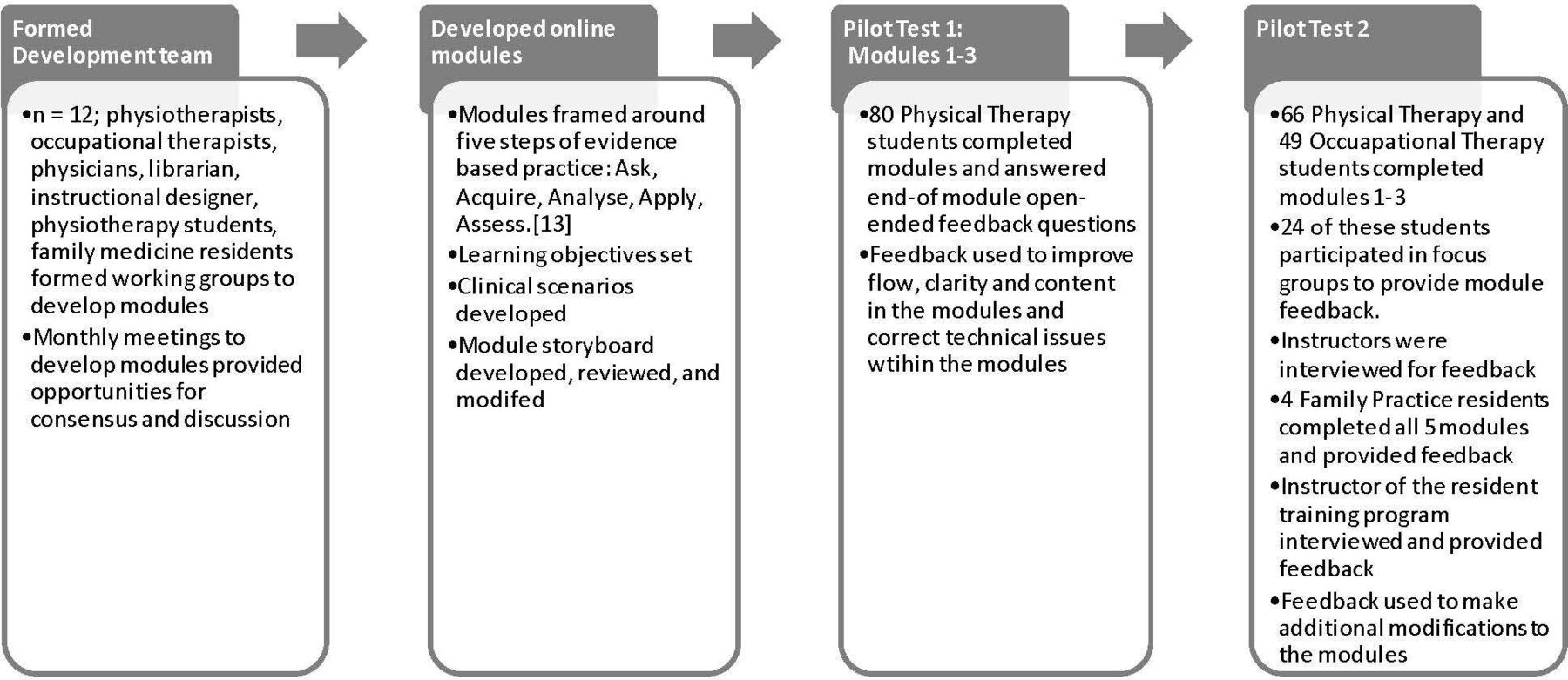
The concept for the West coast Interprofessional Clinical Knowledge Evidence Disseminator (WICKED) modules stemmed from the need for EIHC education for students and clinicians across the healthcare disciplines. Figure 1 briefly outlines the process followed in the development and pilot testing of the modules. Table 1 provides a description of each module, the learning objectives and estimated completion time.
Description of the five WICKED modules, their learning objectives and completion time
{kind=link}
Flowchart depicting the process followed in the development and pilot testing of the WICKED modules. WICKED, West coast Interprofessional Clinical Knowledge Evidence Disseminator.
Clinical scenarios and contexts were designed to resonate with learners across different health professional contexts and emphasised collaborative practice and patient-centred care. Based on the literature review, the team framed the knowledge and skills around virtual patient cases that would engage the learners and give them an example of application in clinical practice. The integration of media elements was essential to engage the learner and provide clinical context, for example, videos, images, audio files, comic strips and patient charts. Modules were designed for online learning, providing maximum flexibility to students and clinicians with regards to how and when the modules could be incorporated into course work and other teaching approaches. Also, they were designed to be used either as stand-alone modules or in conjunction with the EIHC learning already embedded into individual healthcare professional programmes.
Ethical approval was granted by the University of British Columbia Institutional Review Board. The modules were initially pilot tested with a cohort of 80 student volunteers in the Physical Therapy (PT) programme (pilot test 1; figure 1).
The following year, the modules were made available to instructors in the PT and Occupational Therapy programmes (pilot test 2). The instructors gave individual feedback on module content before embedding modules into their core courses (modules were mandatory but not scored). This feedback included comments that the content of modules was good and requests for an increase in comparative statistics in module 3. Student focus groups provided feedback on accessing and navigating through the modules. Their comments were related to the level of completion of the modules, the amount of additional materials accessed, what they liked and disliked about the modules, the effectiveness of the modules on increasing their understanding of EIHC, and whether they encountered any challenges in using, or would like to change anything about the modules. This feedback led to modifications being made to the modules.
Four first-year Family Practice residents were invited to complete the modules as part of their resident training programme while located in rural British Columbia and were each assigned one of the modules to teach to their peers. The development team gathered feedback following a similar remit as the student focus groups. The instructor of this resident training programme was individually interviewed and gave feedback on how the modules were used, the impact of modules on teaching, challenges encountered, satisfaction and whether they would use the modules again.
Feedback from the instructors, student and resident groups (table 2) was categorised into four areas:
Quotes from students, residents and instructor feedback
User perception of module effectiveness
Unlike the students, residents reported that the modules provided them with a review of what they already knew about EIHC, rather than introducing new information. They found this review helpful and good use of their time and the online nature and flexibility was appreciated.
They indicated that time spent on four of the five modules was appropriate given the amount of content; the exception was module 3 (Appraise) that they found time consuming. They stated that the content was informative and the videos well produced, giving the modules a very professional quality.
Neither students nor residents liked open-ended questions. They indicated a preference for checklists, multiple-choice questions and other ways that required less effort to self-evaluate their understanding of content.
Instructor perception of module effectiveness
The residents’ instructor made extensive use of the modules, finding WICKED to be an effective and well-designed tool that they would use again. They found the modules’ design, in which learners progress from learning the basic knowledge and skills of EIHC to having opportunities to apply these knowledge and skills in clinical scenarios, to be highly valuable.
Impact of technical issues on learning
Unlike the students, the resident’s experienced significant technical issues accessing the modules due to working remotely and often during non-business hours. These issues included difficulty in finding the modules within the system, being kicked out of the system, and the enter key submitting a written answer rather than moving the cursor to start a new line of text.
Suggestions for improvement
Learners suggested several ways to improve modules, for example, in terms of content, evaluation and linkages (table 2).
Discussion
Inherent in the process of module development were facilitators and challenges. Facilitators included the breadth of knowledge, expertise and experience of the interprofessional project team related to EIHC, education and clinical practice, which enabled discussions and decisions. The team included educators, clinicians and learners providing a forum to consider issues from various perspectives. The interprofessional composition of the team highlighted the common competencies and allowed for case studies and examples that enable the modules to be relevant across healthcare professions. The various perspectives of the team members led to differences in opinion related to what specific content should be included or highlighted in the modules and which virtual cases might best illustrate learning objectives. Consensus was always arrived at, and modules were produced iteratively.
Feedback from every group provided useful information; for example, module 3 contains 10 scenarios, of which learners are expected to work through one or two that are appropriate to their learning objectives. Lack of clear instructions to learners and instructors led to learners completing more content than expected with the resultant excessive time commitment. As a result of this feedback instructions for this module were improved. Identification of technical difficulties was valuable information that the design team used to improve the experience for all users.
There is a need for further evaluation of these modules. Each step requires a different level of knowledge and skill; therefore, each should be assessed to determine a learner’s competence in EIHC. However, most available assessment tools focus on assessing only one or two steps and none that assess all five steps have had both their validity and reliability established.12 Consequently, we are developing and testing a set of tools that will assess learners’ competence in all five steps of the EIHC model. Valid and reliable measurement of EIHC competence is important for instructors to prepare and train learners to be effective EIHC practitioners in clinical practice; and to demonstrate to respective stakeholders and educational programme accreditors that EIHC competencies are being met.
Conclusions
The use of virtual cases combined with interactive online teaching tools enables interdisciplinary teaching of EIHC, with the advantage of meeting different learner needs in terms of timeliness and content.
It is possible to address some of the barriers to learning core EIHC knowledge and skills through online, virtual patient EIHC modules. Further testing of knowledge and skills gained from the modules is required using a valid and reliable measurement tool.
Data availability statement
All data relevant to the study are included in the article
Ethics statements
Patient consent for publication
Ethics approval
University of British Columbia IRB H16-00749.
Footnotes
Contributors All authors have contributed to all stages, from the design and implementation of the project to the writing of the manuscript.
Funding This study was funded by Teaching and Learning Enhancement Fund, University of British Columbia.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.